Photos of #EndDiabetsStigma around the world
if you would like your photos to appear on the website, please email us a copy.
























Diabetes Initiative Indonesia



Central Coast Health – Paediatric Diabetes Team

Abbott Australia

Leicester Diabetes Centre

 End Diabetes Stigma and Discrimination
End Diabetes Stigma and Discrimination
if you would like your photos to appear on the website, please email us a copy.
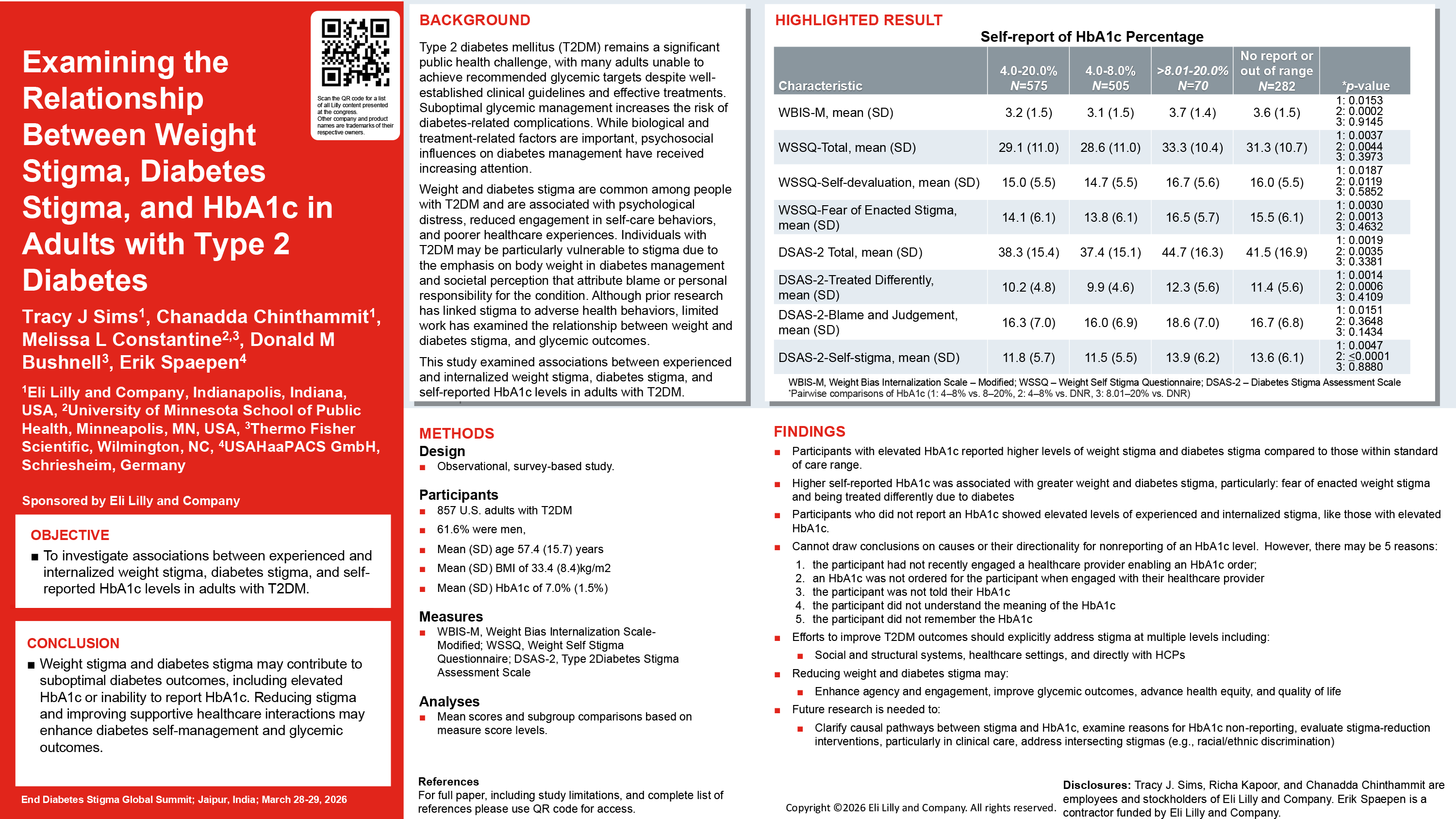
Tracy J Sims, Eli Lilly
Introduction
This study aims to examine the extent to which experienced and/or internalized weight stigma and diabetes stigma may be associated with HbA1c level in adults with type 2 diabetes mellitus.
Methods
A total of 857 participants completed a web-based survey including self-reported demographics, weight, HbA1c, and measures of weight stigma and diabetes stigma, including the Modified Weight Bias Internalization Scale (WBIS-M), Weight Self-Stigma Questionnaire (WSSQ), and the Type 2 Diabetes Stigma Assessment Scale (DSAS-2).
Results
Participants with elevated HbA1c reported greater weight stigma and diabetes stigma than those with an HbA1c level within the standard-of-care range. Exploratory subgroup analysis of participants who did not provide an HbA1c level reported experiencing and internalizing weight stigma and diabetes stigma at similarly high levels as those with elevated HbA1c. Compared to Black non-Hispanic participant’s mean WBIS-M and WSSQ-Total scores, Hispanic participants and White non-Hispanic participants reported greater weight stigma. Hispanic participants endorsed higher DSAS-2 Self-Stigma scores than Black non-Hispanic participants.
Conclusions
Weight stigma and diabetes stigma may be associated with suboptimal diabetes care outcomes measured as elevated HbA1c or inability to report an HbA1c level.
Sims, T.J., Chinthammit, C., Constantine, M.L. et al. Examining the Relationship Between Weight Stigma, Diabetes Stigma, and HbA1c in Adults with Type 2 Diabetes. Diabetes Ther 16, 2137–2156 (2025). https://doi.org/10.1007/s13300-025-01795-8
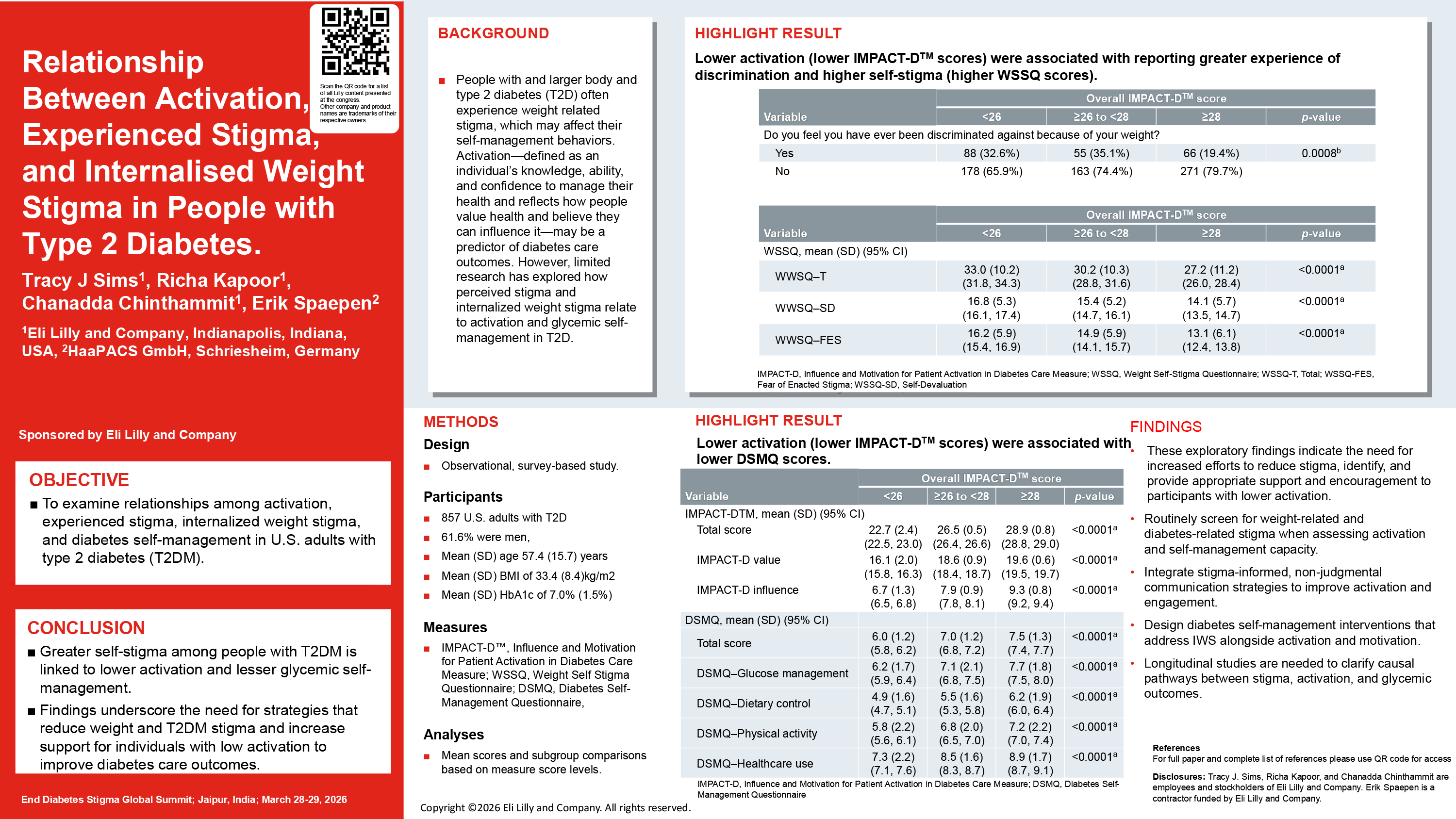
Tracy J Sims, Eli Lilly
Introduction
Activation is associated with disease self-management; limited research has examined the role of perceived stigmatisation in this relationship. We explored links between diabetes and weight stigma, internalised weight stigma, and activation among people with type 2 diabetes (T2D).
Methods
This observational, survey-based study was conducted among 857 US adults with T2D. Mean scores were reported for participant-reported outcome (PRO) measures, including first use in research of the Influence and Motivation for Patient Activation in Diabetes Care measure (IMPACT-DTM), Weight Self-Stigma Questionnaire (WSSQ), Type 2 Diabetes Stigma Assessment Scale (DSAS-2), Diabetes Self-Management Questionnaire (DSMQ), Brief Illness Perception Questionnaire (Brief-IPQ), and questions about perceived weight stigma and discrimination. Additional subgroup analyses were based on total PRO scores.
Results
Participants with lower degrees of activation (lower IMPACT-DTM scores) experienced greater self-stigma (WSSQ scores) compared to those with higher degrees of activation. People with high weight-related self-stigma (WSSQ scores) experienced more self-stigma (high Brief-IPQ, DSAS-2 scores), lower activation, and poorer glycaemic self-management (lower IMPACT-DTM, DSMQ scores) than people with less self-stigma. Higher degrees of self-stigma (high WSSQ and DSAS-2 scores) were reported among people who faced weight-related stigma compared to those who did not.
Conclusions
Greater degrees of self-stigma were associated with lower degrees of activation and poorer glycaemic self-management. The exploratory findings indicate the need for increased efforts to reduce stigma, identify, and provide appropriate support and encouragement for people with T2D who have lower activation.
*This abstract associated with manuscript that has been accepted for publication in Diabetic Medicine.
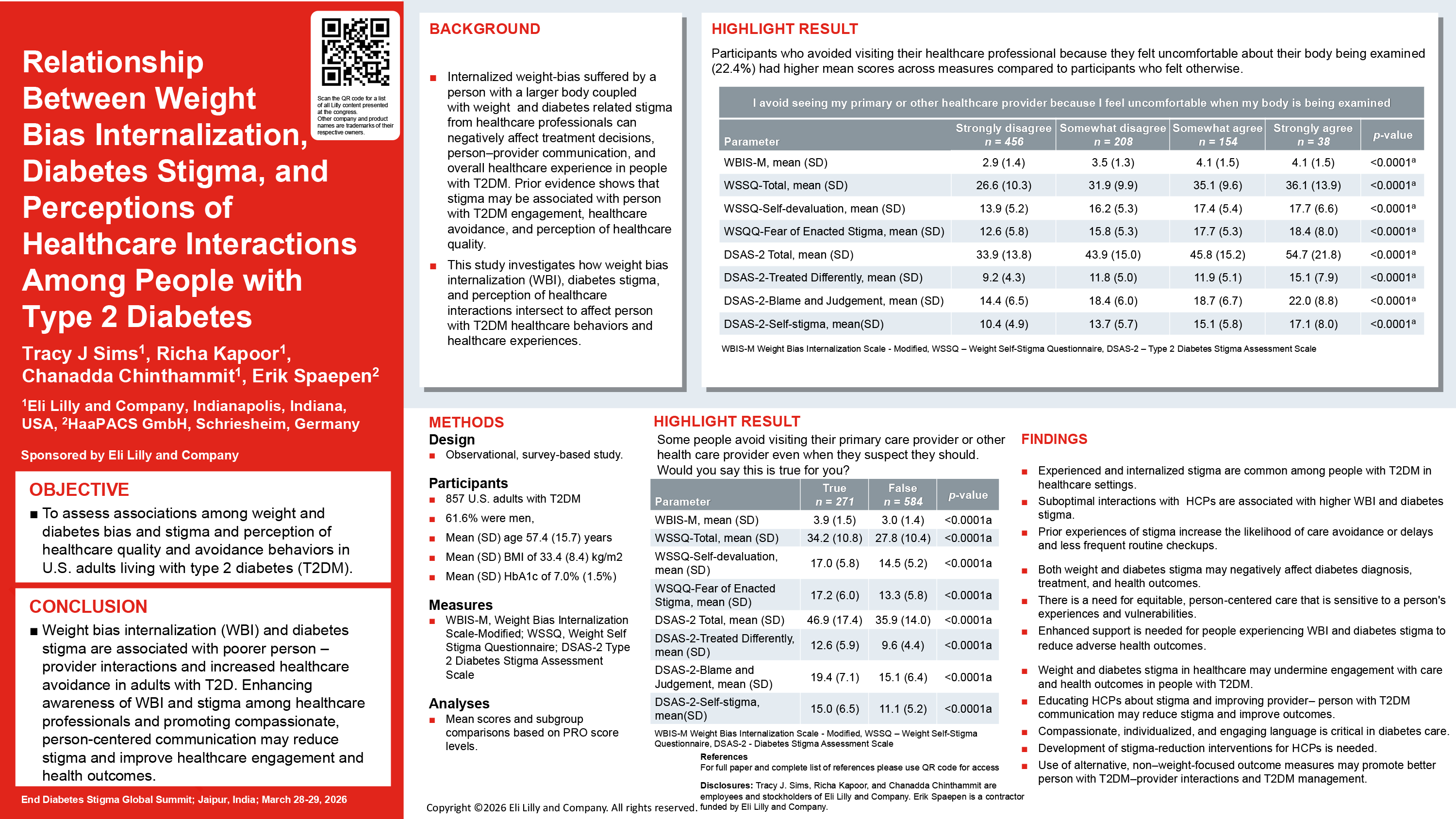
Tracy J Sims, Eli Lilly
Introduction
Weight and diabetes stigma among healthcare professionals (HCPs) may negatively impact treatment decisions, care outcomes, and physician–person with diabetes interactions. We assessed the relationship between weight stigma, diabetes stigma, perceptions of healthcare quality, and avoidance of healthcare among adults with type 2 diabetes (T2D).
Methods
This observational, online survey-based study included 857 US adults with T2D. The survey included perceptions of person-centered care with questions from the Consumer Assessment of Healthcare Providers and Systems (CAHPS) survey, perceptions of provider communication with questions from the Diabetes Attitudes, Wishes, and Needs (DAWN) study, de novo questions assessing participants’ interactions with HCPs, perceived weight stigma and discrimination, and healthcare quality/avoidance delay questions. Mean scores were reported for paricipant-reported outcome measures: Modified Weight Bias Internalization Scale, Weight Self-Stigma Questionnaire, and Type 2 Diabetes Stigma Assessment Scale. Additional analyses were based on CAHPS, DAWN, and healthcare quality/avoidance responses.
Results
High degrees of weight bias internalization (WBI) and diabetes stigma were observed among participants dissatisfied with their overall involvement in their care and those who perceived judgment from the HCP because of their weight. Participants with high degrees of WBI and diabetes stigma were more likely to avoid seeking care, felt uncomfortable with body examinations, and rarely underwent regular health checkups. Those who had suboptimal interactions with their HCPs reported greater stigma.
Conclusions
Increasing awareness among HCPs regarding weight and diabetes stigma and promoting compassionate communication in healthcare interactions may help diminish these forms of stigma, thereby potentially improving health outcomes for people with T2D.
*This abstract from already published paper:
Sims, T.J., Kapoor, R., Chinthammit, C. et al. Relationship between Weight Bias Internalization, Diabetes Stigma, and Perceptions of Healthcare Interactions among People with Type 2 Diabetes. Diabetes Ther 16, 2025–2044 (2025). https://doi.org/10.1007/s13300-025-01786-9
Bernhard Kulzer, Research Insitute of the Diabetes Academy (FIDAM)
| Co-authors: | Laura Klinker, Birgit Olesen, Dominic Ehrmann, Norbert Hermanns, Jens Kröger |
Introduction
Prejudices and lack of knowledge about diabetes are a breeding ground for stigmatization. In this study, we asked people with T1D and T2D about their assessment of the causes of diabetes and the level of knowledge, and how they believe this is perceived by society.
Methodology
Online survey of 602 people with diabetes (PwD) (n = 489 T1D, 58% female, age 56.6 years (13.2), duration of diabetes 30.5 years (17.4), HbA1c 6.7% (2.7), 61% AID system, 9% CSII, 30 MD1; (n = 113 T2D, 23% female, age 65.6 years (11.5), duration of diabetes 19.7.5 years (11.2), HbA1c 7.7% (3.8), 33% insulin, 28% oral, 28% GLP1, 3.3, basal, 2% no oral medication/insulin). Likert scale with 5 response categories from “strongly agree” (5) to “strongly disagree” (1).
Results
Both T1D (3.7) and T2D (3.6) believe that there is too little knowledge about diabetes in society. PwT1D believe that people without diabetes also perceive this to be true with regard to T1D (3.8), while PwT2D do not perceive this to be true for T2D (3.3) (p>0.05). Both PwTD1 (3.6) and PwT2D (3.7) consider that there are many prejudices about diabetes in the general public (n.s.). While PwT1D do not believe their disease is their own fault (4.9), they think that this is often assumed by the general public (2.7) (p>0.01). PwT2D also believe more that T1D is not their own fault (3.4) and believe that this is similarly viewed by society (3.4) (n.s.). Both PwT1D and T2D tend to rate their condition as “severe” (3.7), but believe that their diabetes—especially T2D—is more likely to be viewed as a “mild” condition. Most PwD believe that diabetes is not given sufficient attention in health policy (4.4), but that this is not generally perceived by the public (TD1 3.4; TD2 3.0) (p>0.05).
Discussion
PwD believe that there are a number of knowledge gaps and prejudices regarding diabetes that are only perceived to a limited extent by the general public.
Bernhard Kulzer, Research Insitute of the Diabetes Academy (FIDAM)
| Co-authors: | Laura Klinker, Birgit Olesen, Dominic Ehrmann, Norbert Hermanns, Jens Kröger |
Introduction
Until now, there has been no reliable data on the extent of diabetes stigma in Germany. Therefore, a study was conducted in which people with T1D and T2D were asked about various areas (n = 15) of stigma.
Methodology
Online survey of 602 people with diabetes (PwD) (n = 489 T1D, 58% female, age 56.6 years (13.2), duration of diabetes 30.5 years (17.4), HbA1c 6.7% (2.7), 61% AID system, 9% CSII, 30 MD1; (n = 113 T2D, 23% female, age 65.6 years (11.5), duration of diabetes 19.7.5 years (11.2), HbA1c 7.7% (3.8), 33% insulin, 28% oral, 28% GLP1, 3.3, basal, 2% no oral medication/insulin). Likert scale with response categories 0 (often) – 4 (never).
Results
34% of respondents rated at least one of the 15 situations (items) as “often.” 98% rated at least one of the 15 items as “often,” “frequently,” or “rarely” – only 2% have never experienced a situation of stigmatization. PwD T1 often or frequently report having been pitied because of their diabetes (93.8%), experienced negative comments about their nutrition (81.9%), felt guilty in connection with their therapy results (79%), been questioned by others about their ability at work due to diabetes (74.1%), and concealed their glucose levels due to an expected negative reaction from others (54.1%). In T2D, regret about diabetes was also most common (70.6%), followed by items other than those in TD1: negative comments about nutrition (68%) and physical exercise (63.9%), feelings of guilt about treatment results (63.8%), and being questioned about their ability to perform (56.2%).
Discussion
The extent of stigma experienced is high, with almost all people with diabetes having had such situations. There are significant differences between people with T1D and T2D. However, this study cannot draw any conclusions about the degree of burden caused by this experienced stigma.
Sarina Aryal, University of Calgary
| Co-authors: | Tucker Reed; Saania Tariq |
Background
Homelessness presents a host of barriers for individuals living with diabetes, with stigma being a particularly pervasive issue. A narrative film was created as a knowledge mobilization tool to address the lack of awareness which serves as a key driver of this stigma. The objective of the study was to investigate how a narrative film (Low) impacts diabetes awareness and inspires action among Canadian homeless-shelter workers by exploring their experiences, thoughts, and reflections after watching the film.
Methods
A qualitative descriptive study was undertaken. Data were collected through semi-structured interviews and inductively coded using thematic analysis. Themes were developed from the coded data by linking shared ideas and meanings between them, creating interpretive stories being told through the data.
Results
Six staff participants were recruited from homeless shelters across Canada after they had viewed the film. The use of a narrative film was seen as being more approachable compared to media such as literature or lectures, and the film’s portrayals were seen as accurate and relatable by participants, which facilitated their connection with its subject matter, allowing the messages of the film to resonate deeply. The resonance of these messages inspired participants to be more mindful of those living with diabetes and extend their newfound awareness into their daily work.
Conclusions
The findings of this study highlight potential mechanisms through which a narrative film can be an effective knowledge mobilization tool.
Rose Stewart, Betsi Cadwaladr University Health Board
| Co-authors: | Jane Diggle; Samuel Seidu; Waqas Tahir; Deepa Shanmugasundaram; Charlotte Gordon; Nicola Milne |
Background
The diabetes CARES programme is an anti-stigma initiative aimed at primary care diabetes practitioners in the UK that is being co-developed by a multi-disciplinary team of diabetes healthcare professionals (HCPs), academics and people living with diabetes (PLwD) with support from industry. The vision of the programme is to foster a diabetes care environment where HCPs are equipped to deliver compassionate, unbiased, and stigma-free support, empowering every person living with diabetes to feel respected, understood, and actively involved in their care.
Methods
The programme concept developed during a session focussing on stigma at a Primary Care Technology Network meeting (supported by Abbott) where multi-disciplinary primary care HCPs discussed the sources of stigma within their practice and barriers to providing compassionate care. Each identified barrier was systematically mapped to specific COM-B components (Capability, Opportunity, Motivation) to guide targeted intervention design. The group members rated the proposed solutions in terms of novelty, feasibility of delivery and likeliness of uptake.
Outcomes
The group agreed to co-create and implement a practical, evidence-based HCP training toolkit that is underpinned by the COM-B model and principles of compassionate care. The CARES acronym at the core of the programme covers fundamental elements of compassionate, anti-stigmatising healthcare (Communication, Awareness, Reflection, Empowerment, Support), while additional ‘bolt on’ elements cover specific key timepoints in a person’s diabetes journey (e.g. diagnosis, insulin initiation) as well as vulnerable populations (e.g. minoritized ethnic communities, people with diabetes distress). Uptake of the programme will be maximised by further application of behavioural science techniques, using elements of the behaviour change wheel.
Evaluation will use pre- and post-training assessments of HCP attitudes and confidence, alongside feedback from people with diabetes to assess perceived stigma reduction and greater trust in care.
Sasha Delorme, Unified Diabetes Advocacy and Awareness
| Co-authors: | Maya Pajevic; Stacey Dickinson |
Background / Context
Stigma and discrimination toward Indigenous people living with type 1 diabetes (T1D) intersect with colonial legacies, systemic racism, health system mistrust, and inequitable access to culturally safe care. Biomedical models often overlook Indigenous ways of knowing, overlooking cultural narratives of resilience, kinship, and collective healing central to Indigenous worldviews. These omissions perpetuate mistrust in health institutions and reinforce historical trauma. Current national diabetes frameworks, while increasingly inclusive, remain limited in addressing the root causes of social and structural stigma that perpetuate disparities in diagnosis, management, and mental health outcomes for Indigenous communities living with T1D.
Opportunities
Transformative possibilities lie in integrating Indigenous knowledge systems into national diabetes strategies and in expanding cross-sector collaborations among governments, Indigenous organizations, and academic centers. Digital health tools and community-driven innovation, such as co-designed applications or remote monitoring programs led by Indigenous clinicians, offer potential to reimagine culturally grounded diabetes care. Policy reform aligning with the Truth and Reconciliation Commission’s Calls to Action and the United Nations Declaration on the Rights of Indigenous Peoples Act can embed accountability and sustain momentum.
Challenges
Persistent intersectional stigma rooted in racism, socioeconomic inequity, and chronic disease bias has the potential to complicate both engagement and program sustainability. Evaluation frameworks rarely capture cultural safety, and funding cycles often constrain the implementation of longitudinal, community-centered interventions. Balancing global research standards with local autonomy remains a fundamental tension.
Recommendations
Future efforts should establish Indigenous-led research and inter-sectoral care networks focused on lived-experience metrics, secure sustained funding for intergenerational education initiatives and mentorship, and embed stigma-reduction targets within health equity performance frameworks. Co-creation across health, education, and policy sectors can normalize Indigenous leadership in diabetes advocacy and data sovereignty, embed cultural safety standards, and recognize Indigenous data governance as foundational to equity in T1D care.
Recommendations
This work is led by an independent Indigenous research professional with type 2 diabetes, caring for her son living with T1D, and two other patients living with T1D, whose narratives shaped the analysis of stigma, identified systemic gaps, and co-developed culturally relevant recommendations.
Elizabeth Holmes-Truscott, ACBRD, Diabetes Victoria and Deakin University
| Co-authors: | Meaghan Read; Ashley Ng |
Background
Community involvement (CI) is increasingly recognised as essential for prioritising what matters to people with lived experience, selecting methods and interventions that are acceptable to community, and enhancing the impact of diabetes research and health services. Addressing stigma and power imbalances have been identified as key enablers of CI. The international consensus on diabetes stigma further emphasises the responsibility of researchers and health professionals to adopt stigma-free practice, including person-first, strengths-based, and non-stigmatising language.
Opportunities
When lived-experience, clinical, and academic expertise are recognised as equal (while qualitatively distinct), CI becomes a mechanism for the redistribution of leadership and embedding stigma-free practice. Language is central to this process because it reflects attitudes, values, and intentions. The diabetes #LanguageMatters movement demonstrates the influence of words in shaping perceptions and interactions, and highlights the need for neutral, respectful, person-first communication that centres lived-experience expertise and preferences. Embedding these principles, and established preferred-language recommendations, within CI offers an opportunity to strengthen partnership approaches and support stigma-free practice.
Challenges
People with diabetes report stigma as a barrier to research / health service involvement, potentially exacerbated by inconsistent use of person-first and strengths-based language. Despite the growing momentum of CI within diabetes research and health service improvement, there remains limited evidence on how diabetes stigma is addressed or preferred diabetes language is identified and implemented. Well-intentioned CI initiatives may inadvertently reproduce hierarchies when non-recommended terms in diabetes, such as “consumer engagement” or “patient partners”, recentre institutional authority and reinforce unequal roles.
Recommendations
Co-develop partnership language that avoids hierarchical framing and fully embeds lived-experience leadership and co-ownership, reflecting principles and processes across governance, decision-making, and authorship. Require journals and funders (and all submissions) to adopt stigma-free communication standards and recognise lived-experience expertise. Evaluate language use, preference, and impact, across all research and service improvement.
Bernhard Kulzer, Research Insitute of the Diabetes Academy (FIDAM)
Abstract
The German Diabetes Society (DDG) and diabetesDE (an organization for people with diabetes) are planning a multi-year campaign aimed at reducing both knowledge deficits and prejudices regarding diabetes as a disease and people with diabetes.
The public perception of diabetes as a minor, “mild” and self-inflicted disease (especially type 2 diabetes) prevents society from taking responsibility for the disease and taking measures against the stigmatization and discrimination of people with diabetes. The campaign is based on the principle that “diabetes should be treated well, not judged.” Together with partners from science, health, business, civil society, and diabetes communities, the aim is to create a powerful movement that raises awareness of diabetes, demystifies it, and empowers people with diabetes. The campaign’s goals are based on the content of the DDG’s “Diabetology Agenda 2030,” which outlines various areas of action for improving the perception and treatment of diabetes. Each year, a campaign focus is chosen (“Prejudices and knowledge deficits about diabetes,” “Giving people with diabetes a voice,” “Prevention of diabetes”). The aim is to involve a large number of institutions, professional associations, and organizations via the Diabetes Network Germany in order to reach a broad public and develop strategies for different target groups and settings. An evaluation of the campaign is planned. The campaign is scheduled to start in 2026 and will be implemented using a multi-channel approach. The content of the campaign ranges from advertisements, poster campaigns, commercials, and videos to discussion forums and opportunities for personal encounters. The goals and content of the campaign will be presented.
Renza Scibilia, Breakthrough T1D
| Co-authors: | Jane Speight; Bryan Cleal; Jane Dickinson; Jazz Sethi |
Background
War metaphors have been used in healthcare for decades, particularly regarding cancer and viruses. They are increasingly common in diabetes. Apparently, we are waging a “war on diabetes” due to the “diabetes explosion”, with increasing imperative to “tackle”, “combat”, “fight harder”, “beat”, “conquer” and “defeat” diabetes. However, this well-intentioned messaging has unintended consequences. The continuous “battle” feels insurmountable and exhausting, leading people to fear blame for not trying hard enough. It amplifies the already negative impacts of diabetes on physical and mental well-being. Evidence shows people with diabetes spend 77 minutes daily thinking about their condition, e.g. checking glucose levels and managing variations in routine, hormones, activity, food, stress, weather, illness, and medications. People with type 1 diabetes, women, and those using advanced technologies think about their condition even more, with stigma and mental health risks amplifying this burden. This is not a “fair fight”.
Opportunities
The opportunity lies in reframing messaging to acknowledge this reality and reposition people with diabetes as experts, deserving of our support, doing a job none of us would ask for. The opportunity is to harness “contact theory” in campaigns that empower without burden and support without stigma.
Challenges
There is intuitive appeal in countering the entrenched “diabetes epidemic” messaging, of the past 25 years, with military metaphors, to drive attention and fundraising. Alternative approaches may seem risky. Yet, breast cancer advocacy succeeds through strong societal narratives that women deserve support, enabling sustained cross-sector partnerships.
Recommendations
Rather than positioning the diabetes community to “fight” policymakers for limited resources, and requiring partners to “choose sides”, we need support-focused advocacy harnessing authentic collaboration and sustainable partnerships. Diabetes advocacy needs to centre people with lived experience as expert leaders and valued members of society deserving support. We need co-designed campaign frameworks and accountability mechanisms promoting partnership-focused advocacy.
Jane K Dickinson, Teachers College Columbia University
| Co-authors: | Diane Scherer; Chris Bright; Dessi Zaharieva; Matthew Garza |
Background / Context
The language movement in diabetes can be confused with “political correctness.” Sometimes it seems like simply being told not to use certain words, and feeling like one is “wrong” or “incorrect” when slipping up.
Opportunities
The language movement in diabetes is an opportunity to lead by example and teach people why the words they use matter. It is possible that changing the language of diabetes could lead to improved behavioral, emotional, and health outcomes for people with diabetes.
Challenges
Resistance to change abounds, and it’s always easier to keep doing what we are used to, especially if we don’t see the meaning behind the change.
Recommendations
Show health professionals, family, friends, the public, and those living with diabetes that person-centered, strengths-based, and engaging language matters and encourage them to adopt it as well as teach others to do the same.
Polina Kukhar, Columbia University
Abstract
Growing up in the era of social media, I, like many young adults newly diagnosed with type 1 diabetes, instinctively turned online to make sense of a condition that arrived overnight. Within hours, I was learning from other people’s glucose graphs, pump placements, and routines. These platforms offered belonging and a crash course in diabetes management that no clinic could deliver as quickly.
But working inside a major social-media company revealed the other side of the algorithm: the content that rises is rarely the most accurate or mentally sustaining—it’s whatever performs best. Increasingly, that means videos showcasing perfect time-in-range percentages, idealised routines, elite athletes with sponsorships, and an aesthetic of control that is neither universal nor attainable.
Nowhere is this clearer than in endurance-sport communities. As a marathon runner with T1D, I often saw creators posting flawless glucose lines during training cycles—lines physiologically improbable without expensive tech, extreme trial-and-error, or constant monitoring. These posts quietly redefine what “success” looks like, implying that those who struggle simply lack discipline. In reality, most people do not have access to the latest automated insulin delivery systems, personalised nutrition support, or the mental bandwidth to chase perfection while managing a chronic condition.
The result is a modern form of diabetes stigma shaped by algorithms: a pressure to perform health publicly, to prove competence through numbers, and to appear in control even when the condition itself resists control. That pressure affects caregivers, too, who compare their child’s data to curated examples that have been edited, filtered, or amplified.
These dual perspectives– living the diagnosis and understanding the mechanics behind what gets seen– make clear that the issues lie in the incentives driving social media. If platforms and technologies are to reduce rather than reinforce stigma, they must elevate nuance, support, and lived experience over perfection.
One of the things I learnt when studying Neurolinguistic Programming (NLP) was the concept that behind every decision is a positive intention. Which can also be restated as nobody deliberately makes a bad decision. Which means that everybody is doing the best they can at the time with the knowledge, experience and resources they have available to them.
Alex St. John, Diabetes Action Canada
| Co-authors: | Emily Burke-Hall; Linxi Mytkolli; Robin Lucciantonio; Peter Senior |
Background / Aim(s)
Cell therapy and islet transplantation have changed what is possible for some people with type 1 diabetes, but most information is highly technical or framed as a “miracle cure.” This creates confusion, unrealistic expectations and stigma about who is “sick enough” or “deserving” of advanced therapies.
As part of the Diabetes Action Canada Research-to-Action Fellowship, in partnership with the Alberta Diabetes Institute, this project aims to explain 26 years of islet transplant progress in plain language so people can understand what cell therapy can and cannot do in real life.
Methods
Two Fellows, Alex (lived experience) and Emily (loved experience), worked with endocrinologist Dr. Peter Senior and diabetes educator/researcher Robin to review key milestones from the Edmonton Protocol to today.
A co-design session with over two dozen people living with type 1 diabetes explored their fears, questions and information gaps about cell therapy, including worries about risk, eligibility, cure language and long-term outcomes. In parallel, more than 12 islet transplant recipients shared brief testimonials about life before and after transplant.
These insights were translated into “Cell Therapy 101: 26 Years of Progress in Type 1 Diabetes,” a plain-language infographic series explaining islets, type 1 diabetes and islet cell transplants, highlighting benefits and current gaps. The series is shared as a free digital carousel with a QR code so people can easily follow ongoing research and updates.
Outcomes (achieved or expected)
Early feedback from transplant recipients, community members and clinicians suggests the series makes complex science understandable and honest, reduces fear of asking questions and supports more realistic expectations about who cell therapy may be for. Expected outcomes include more informed clinic conversations and better alignment between people’s hopes and the actual goals of transplant programs.
Lessons Learned (for scaling / adaptation)
Blending clear visuals, simple language and real-life stories shifts cell therapy discussions away from hype or fear and toward grounded, person-centred dialogue. Partnering Fellows with a research institute ensured both accuracy and relevance. The format is adaptable for other regions and emerging therapies by pairing local clinical teams with community storytellers.
Leana Satim, Gold Bug Interactive
Abstract
The Game Plan Comic is a free, web-based comic created thanks to a grant from Breakthrough T1D Canada, and in partnership with McGill University. Our multi-media education company, Gold Bug Interactive, consulted with children and adults living with T1D, as well as doctors, and mental health professionals to create this comic, which is intended as a resource to support mental health for newly diagnosed T1Ds aged 9+ and their families. The bold and intense images mimic the strong emotions that often accompany this diagnosis, and the final message is one of hope. Our daughter, who is now 11 years old, was diagnosed with T1D 3 years ago, and she was an integral part of the creation of this comic. The intention is to help youth like our daughter feel seen and supported, to offer hope and also some ideas for emotional healing following diagnosis. This web-based comic is also a resource that can be shared with classmates, educators, peers, coaches and teammates to promote understanding, education, awareness, and to help remove the stigma of living with this auto-immune disease in an engaging and entertaining way. Starting in 2026, this comic is being formatted for print so that it can be included in Breakthrough T1D Canada’s Bag of Hope, which is distributed to newly diagnosed youth, so as to maximize the impact of this resource. Here is a link to the web comic: https://thegameplancomic.goldbuginteractive.com/
Zoe Khalap, Hypoglycemia Awareness, LLC
Abstract
This abstract presents measurable, successful results of a 13 year old, non-profit, multi-disciplinary, low-cost and low-tech intervention that was developed by a PWD with the goal of reducing diabetes stigma associated with hypoglycemia in public settings. Hypoglycemia is one of the leading fears of people living with diabetes, leading some to take self-harming decisions to reduce insulin therapy delay treatment and avoid the risk of hypoglycemia in public. Through education initiatives aimed at first responders regarding the signs and symptoms of mild to moderate hypoglycemia, the incidence and impact of severe hypoglycemia and the negative harm of stigma were reduced. By normalizing the conversations around a known risk to public safety, efficiency and productivity, the comfort level and readiness of first responders increased, thus creating a more understanding and supportive community for people living with diabetes in public settings. Tools used are physical reminders, posters, buttons, stickers and online educational resources. See www.hypoglycemiaawareness.org
Linxi Mytkolli, Diabetes Action Canada
| Co-authors: | Laurie Lepine |
Abstract
Diabetes stigma shows up in weight-biased clinical encounters, dismissed concerns from Indigenous and racialized patients, minimized mental health, and inaccessible language that keeps research out of community hands. Patient engagement is often invited into this system but rarely given power to change it.
The Research-to-Action Fellowship, created by Diabetes Action Canada, builds a structural response to stigma by training and paying patient partners to lead knowledge mobilization projects that directly challenge discriminatory narratives and practices in diabetes care.
Co-designed with 18 paid patient partners from the Collective Patient Circle, the nine-month Fellowship provides honoraria, bi-weekly training, mentorship, and travel support. In Year 1, eight Fellows with lived, loved, learned, and laboured experience partnered with four organizations (Obesity Canada, diaTribe, Access Alliance, National Indigenous Diabetes Association). They led co-design sessions with over 60 patient partners from Indigenous, racialized, disabled, and equity-denied communities and translated 26 peer-reviewed papers into community-informed, anti-stigma tools. In Year 2, ten Fellows are mobilizing over 100 additional papers with five new global partners. The Fellowship has received over 120 applications from people aged 16 to 88 across Canada and internationally.
Year 1 products include Indigenous self-advocacy flashcards (including Braille), comics that “flip the script” in shaming clinic visits, culturally relevant vignettes, and mental health infographics in plain language and French. These tools are now used in clinics, trainings, and community events. Fellows have presented at national conferences, including the first fully lived- and loved-experience-led panel at the Diabetes Canada Conference. A formative evaluation using the RE-AIM framework shows increased confidence and leadership among Fellows, while partner organizations report expanded capacity to address stigma through patient-led KM.
Stigma is upheld by structures, not just attitudes. A structured, compensated Fellowship centering those most affected by diabetes stigma can shift research hierarchies, redistribute expertise, and generate practical tools that counter stigma in everyday care. The core model—co-design, paid leadership, structured training, and anchored partnerships—is adaptable to other conditions and countries.
Linxi Mytkolli, Diabetes Action Canada
| Co-authors: | Ryan Hooey; Rosan Wesley |
Abstract
Indigenous people living with diabetes often face racism, stereotyping and rushed appointments in colonial healthcare systems. It can be hard or unsafe to speak up when you do not understand something, need urgent support, or do not want to discuss a topic. As part of the Diabetes Action Canada Research-to-Action Fellowship, in partnership with the National Indigenous Diabetes Association, this project aimed to co-create simple, portable flashcards that support Indigenous people to advocate for themselves in clinic, hospital and community settings.
Two Indigenous Fellows with lived experience of type 1 and type 2 diabetes co-led the project with an all-Indigenous design group and an Indigenous artist. Drawing on four co-design sessions with over 60 community members from across Canada, the team listened to stories about difficult healthcare visits and the phrases people wished they could say out loud. Together they drafted, tested and refined eight colour-coded self-advocacy flashcards. Each card pairs a short, plain-language statement on the front (for example, “I need a sugary drink right now. It is urgent,” or “Could you please explain that differently? I did not quite understand.”) with more information and a QR code on the back.
The flashcards are now available as free printable and digital resources through the National Indigenous Diabetes Association and Diabetes Action Canada, and they have been downloaded tens of thousands of times. Early feedback from Indigenous patients, families and providers suggests that the cards: help people name their needs more clearly, create safer boundaries in appointments and prompt more respectful, two-way conversations. We expect increasing use of the cards in clinics, hospitals, diabetes programs and community education.
Making advocacy tools small, visual and co-written with community transforms abstract ideas like “self-advocacy” into specific, usable sentences. The flashcard format travels easily (in pockets, wallets and phones) and can be adapted with other communities by co-creating new phrases and designs rooted in local languages, teachings and realities.
Linxi Mytkolli, Diabetes Action Canada
| Co-authors: | Noor Zehry; Diane Finegood; Laura Syron; Kim Fletcher; Collective Patient Circle |
Abstract
Diabetes stigma is often felt as personal shame but is produced and reinforced by systems, policies and narratives. As part of the “Changing the Conversation” initiative, we sought a practical way to help people with diabetes and decision-makers see what sits below the surface of both stigmatizing and supportive experiences and imagine alternatives that move from harm to help.
The work began when Diabetes Canada engaged the SFU Morris J. Wosk Centre for Dialogue to undertake a deeper exploration of the experiences of people with diabetes using, among other methods, an iceberg model. The Centre analysed responses to a national Diabetes Canada stigma survey and conducted interviews with people living with different types of diabetes. These data informed an initial iceberg model linking what people experience “above the waterline” with deeper structures and mental models.
Diabetes Action Canada then joined the project, engaging its Collective Patient Circle, a governance body of paid patient partners, and recruiting additional participants with lived and loved experience. In a facilitated session, Circle members reflected on words that describe diabetes stigma and what the opposite would feel like. Using an iceberg template, we mapped experiences across domains including self, home, healthcare, education, media, the diabetes community and social services, and co-created paired “stigma” and “supportive” icebergs. The visible tip shows everyday interactions; submerged layers describe beliefs, policies and practices that either reinforce stigma or enable dignity. These have been translated into a series of visual “stigma iceberg” graphics.
The graphic icebergs are prototypes that will be presented for the first time at the Stigma Summit. We expect them to spark dialogue about how stigma and support operate across levels, help participants externalise stigma from “my fault” to “our systems” and ground conversations about what needs to change above and below the surface. Summit feedback will inform refinement and evaluation of the tool in clinical, community and research settings.
Combining survey data, interviews and co-design with people with diabetes makes systems thinking more concrete and emotionally safer. The iceberg framework appears adaptable to other conditions and contexts by repeating this process with local communities and institutions. This work was financially supported by Diabetes Canada.
Vasco Costa, William James Center for Research
| Co-authors: | Tânia Brandão |
Abstract
I was diagnosed with Type 1 diabetes at the age of 23, at a time when I knew very little about the condition and even less about the stigma associated with it. My initial symptoms included persistent thirst, frequent urination, and unexplained weight loss. After discussing these symptoms with my physician, she recommended that I check my blood glucose at a local pharmacy. Despite having fasted that morning, the reading was 350 mg/dL. I was instructed to proceed directly to the hospital, where I was admitted for a week. This moment marked the beginning of a profound period of adjustment, learning, and reconstruction of daily life, which later motivated my engagement in scientific research and ultimately my doctoral trajectory.
In the months following my diagnosis, I encountered several forms of stigma and misinformation that provoked significant emotional distress. Comments such as “you must have eaten too many sweets,” “don’t eat that,” or “you need to be more active,” as well as jokes like ” he seems a drug addict,” reflected widespread misunderstandings about the condition. I also experienced visible discomfort or avoidance from others in public spaces when checking my glucose or administering insulin. Although these experiences were challenging, they eventually strengthened my commitment to addressing misconceptions and communicating openly about diabetes.
Even today, I continue to encounter remarks that underestimate the complexity of daily management. Statements such as “with a sensor and a pump, it must be easy now” overlook the invisible demands and side of the condition: dysfunctional sleep, continuous vigilance, anticipation of glycemic variability, and the substantial psychological burden.
In sum, these experiences evidence the importance of continued efforts within the diabetes community to promote awareness, enhance public understanding, and effectively challenge stigma.
Phyllisa Deroze, Independent Presentation
Abstract
Beyond the Vial is a compelling one-woman performance written and performed by Phyllisa Deroze that traces her journey with diabetes and the hidden burdens that shape it. It begins with Deroze stepping onto the stage singing a haunting, reflective song that captures the heaviness of life with diabetes—a weight that is often silent, unseen, and carried alone. This musical entry sets the emotional tone for a storytelling experience grounded in truth, resilience, and revelation.
Through expressive storytelling and character shifts, Deroze guides the audience through the years she lived under a misdiagnosis, exposing how stigma and assumptions can distort medical care. She reenacts clinical encounters where her symptoms were overlooked, family moments where misunderstanding deepened her isolation, and reflective internal conversations. By giving voice to these experiences, she reveals how diabetes stigma not only comes from the outside but can also be internalized in painful, lasting ways.
The brief, yet impactful, performance highlights how stereotypes—particularly those aimed at larger bodies, Black bodies, and all bodies that are othered—can shape medical decisions, silence people in need of care, and delay proper treatment.
Beyond the Vial invites audiences to deepen their awareness of the complexities of managing diabetes, extend compassion to those bound by the daily cadence of blood-sugar checks, and push for a future grounded in empathy and understanding.
Wajeeha Cheema, Diabetes Action Canada
| Co-authors: | Maryann Maloney, Saira Khan-Gallo, Linxi Mytkolli |
Abstract
For too long we’ve navigated the challenges of living with diabetes, witnessing gaps in research, especially for women. Our story highlights the need for research and care that directly impacts women directly through lived experiences, addressing hormonal challenges, and life stage complexities. Through these stories we aim to ensure that the voices of women and gender diverse people with diabetes help guide meaningful changes in science, policy, and care.
This project brings together stories and art from women and gender-diverse people living with diabetes — stories of care, connection, and the everyday realities of navigating health at every life stage. In research and in practice, women often get reduced to data points without the context of the lives we’re actually living being taken into consideration.
What we want you to know is that these stories show women are complex. Our hormones, emotions, caregiving roles, stress, infertility, menopause, pregnancy, socioeconomic status, and aging — all of it influences our diabetes. Aging kinda snuck up on many of us, they didn’t expect
that one! And the fact is the research hasn’t kept up with this reality. What we need is research that helps women with diabetes not just live longer, but live well.
Research has shaped diabetes care for decades — yet women’s experiences remain underrepresented. These stories aren’t small or isolated. They repeat and form patterns. When patterns show up in real lives, they deserve attention in research. What we hope this book sparks is a shift — a shift toward seeing women not as outliers or variables to control, but as whole people whose voices should shape the questions we ask. Because we can’t fully understand diabetes and hormonal shifts without understanding women. We can’t meaningfully support women’s health if their lived experience isn’t centered from the start.
We are creating a storytelling book to share these lived experiences with others so they feel heard, to raise awareness about hormonal health and diabetes in general, and to advocate for more empathetic, patient-centered care in healthcare.
Substantial evidence supports the need for such an approach. And we plan to intertwine these evidences with the truths that were shared.
These stories are the heartbeat, the message, and the purpose. We hope this book helps research finally reflect real women’s lives, and encourages clinicians and policymakers to recognize that behind each chart lies a full human life — deserving of empathy, understanding, and better care.
Linxi Mytkolli, Diabetes Action Canada
Abstract
This story starts with a single word that is often treated like a compliment and a warning at the same time: “advocate.”
In this talk, I explore how diabetes stigma is not only about blood sugars, weight or complications, but also about who is allowed to speak, how and at what cost. As a racialized woman living with diabetes who works in patient engagement and policy spaces, I have been praised for being “brave” and “passionate,” and in the next breath told I am “too emotional,” “too close to the issue,” or “not objective.”
These comments are rarely about competence. They are about power and control. They reveal who can advocate without penalty (often white, male, professionally distant) and who is punished—subtly or openly—for naming harm. The talk links this to everyday diabetes stigma: who is believed in hospital rooms, who is labelled “non-compliant,” whose pain is minimized, whose lived experience is treated as anecdote rather than evidence.
I argue that advocacy is already present in every “engagement” space: when someone asks for plain language, insists on being paid, or questions who a system was designed for. Advocacy only becomes a “dirty word” when it stops being decorative and starts being disruptive—when it challenges structures rather than just softening their edges.
The talk invites people with diabetes to reclaim “advocate” as an identity rooted in survival, community and responsibility, not in being difficult. It calls on institutions to stop demanding that people shrink, soften or depersonalize their truths in order to be included. Neutrality is not always a virtue—especially in systems that were never neutral to begin with.
Linxi Mytkolli, Diabetes Action Canada
| Co-authors: | Matt Larsen |
Abstract
Low and its sequel, Low Priority, bring to life what it means to live with diabetes while experiencing homelessness and trying to survive systems that treat you as an afterthought.
In Low, we follow Bobby, a man trying to manage his diabetes while navigating shelters, scarce resources and the constant fear of running out of insulin. Alongside him is Annika, an emergency shelter staff member working in the middle of the opioid crisis, caught between compassion and a system that offers very few real options. Their story is interrupted and deepened by insights and recommendations from a diabetes specialist and from people who have lived this reality themselves.
Low Priority picks up the story from another angle. It shows how an overburdened health system can make diabetes care feel negotiable, “optional” or simply too complicated to prioritise when someone does not have stable housing. The film asks viewers to confront how policies, triage decisions and stigma about substance use and homelessness shape who is seen as worthy of care.
Together, the two films show that the problem is not individual “compliance,” but structures that make safe diabetes care nearly impossible. They invite viewers to sit with the discomfort of seeing their own assumptions on screen and to imagine what it would look like for diabetes care to centre dignity, safety and humanity for people who are unhoused.
These stories are not hypothetical. They are grounded in community-based participatory research with people who live at the intersection of diabetes, homelessness and social disadvantage, and they were created to spark honest conversations and concrete change.
Two narrative short films that blend scripted drama with documentary-style commentary. Low and Low Priority combine acted scenes, realist dialogue and visual storytelling with on-screen reflections and recommendations from people with lived experience of diabetes and homelessness and from a diabetes specialist.
Cameron Keighron, International Diabetes Federation of Europe
Abstract
Living with type 1 diabetes has been shaped as much by the condition itself as by the stigma I encountered within the healthcare system that was supposed to support me. I remember the appointment that would define eight years of my life, beginning with the words, “I don’t trust you with your diabetes.” From then, subtle and not-so-subtle judgments were woven into routine clinical conversations, where questions were asked with assumptions, my concerns minimised, and complications were framed as personal failures rather than outcomes influenced by access or circumstance. My interactions with my endocrinologist consistently centred on what I was not doing, how I supposedly didn’t care enough or try enough, and the unspoken conclusion that I did not deserve help, just shame.
Living in a rural community amplified this through limited education, scarce peer support, and fewer opportunities to build trusting relationships. This stigma & shame had consequences. With a condition I struggled to manage and a doctor who blamed more than empowered, I spent most of my young adult life with blood glucose levels that constantly felt out of “control”. The despair and anger I directed towards myself were frightening. I felt like I was “losing”
During COVID-19, I received a letter telling me I had significant levels of retinopathy and needed urgent treatment. Something that could have been avoided was now coming true. However, it became a turning point in both my health and my sense of agency. Seeing my vision threatened reignited my purpose. Moving from blaming me, I recognised the systemic issue: young adults are often labelled “non-compliant,” “difficult,” or “careless,” when in reality we face complex transitions, geographic barriers, and a healthcare culture that misunderstands our lived experience.
Today, I work to reshape clinical expectations and create environments where empathy replaces judgment, so no young adult feels shamed into silence.
Cyrine Farhat, Positive on Glucose
Abstract
I am loud about having Type 1 diabetes, deliberately loud. I speak openly in public forums, in policy spaces, and across my advocacy work. I use my voice because silence has harmed our community for too long. Yet even with all this noise, there is a quieter truth I live with every day. Despite how visible I am, I still hide so much. I hide my highs to appear competent at work. I hide my lows to be the strong mother I’m expected to be. I smile through exhaustion to be a loving wife. I show up no matter what my blood sugar looks like because perfection is the version of me that the world seems most comfortable with. People see the polished image: the woman who “does it all,” the advocate always in control. They don’t see the burnout, the fear, or the cost of carrying a picture-perfect facade. And behind all of this sits a deeper layer of grief and trauma that shaped my life long before anyone knew my advocacy. I lost my baby at 35+5 weeks to undiagnosed pre-eclampsia, only to be blamed within minutes because “you have diabetes.” I lived through the economic collapse, the Beirut blast, and a war that turned me into an internally displaced person in my own country. I lost my home. I lost everything familiar. I had to rebuild my entire life at 34 while managing a condition that never grants a day off. These experiences taught me that the silent burden of Type 1 diabetes doesn’t exist in isolation. It grows heavier in times of crisis, and stigma only sharpens its edges. I share this story because being loud doesn’t mean being untouched. For many women like me, strength isn’t in pretending; it’s in telling the truth, even when our world has already been turned upside down.
Nura Seidu, Diabetes Youth Care
Abstract
I salute you, my lovely kings and queens. Today, I want to open a small window into my life, my journey living with Type 1 diabetes. I call this journey “Through Stigma and Struggle, I Found Courage and Self-Awareness,” because that is exactly what it has been: a quiet fight that shaped me in ways I never expected.
When I was diagnosed with Type 1 diabetes at just 16, it felt like my whole world shifted overnight. Suddenly, I wasn’t only learning how to check my blood sugar or take insulin… Suddenly, I wasn’t only learning how to check my blood sugar or take insulin; I was learning how to live with a condition that most people around me didn’t understand.
The questions came quickly:
“Are you sure you can eat that?”
“Did you get it because of too much sugar?”
But what hurt more were the judgments, long stares, whispered comments, or the assumptions hidden behind “concerned” looks. In my Ghanaian community, many people believed diabetes was either for the elderly or a punishment for poor lifestyle choices. I was neither old nor careless. Yet, somehow, I found myself carrying the weight of their misconceptions.
So quietly, I began to shrink into myself.
I hid my insulin pen.
I said no to school trips.
I avoided explaining myself because the explanations came with more judgment.
Even at home, questions stung me deeply:
“Are you sure it’s not from your eating habits?”
Those words cut in a way no needle ever could. And little by little, I began to feel ashamed of something I did not cause – something that was simply part of my body.
But life has a way of placing the right people in your path.
My turning point came when I met Kwesi a young man living with diabetes who carried himself with unapologetic confidence. He didn’t hide his diagnosis. I hid my insulin pen. He owned it. And for the first time, I saw someone who looked like me, walked like me, and faced what I faced – standing tall.
Through him, I found a youth support group. I still remember my first day there: sitting in a room where nobody asked “Why?” Nobody judged. Nobody doubted. We just understood each other.
We laughed about our injection mishaps.
We shared stories about scary nights in the hospital.
We cried about fears we had never spoken out loud.
In that room, for the first time in a long time, I felt human again. “Seen.”
That experience changed me.
It pushed me to speak up. I stopped hiding and started sharing my story on social media, in classrooms, in the mosque, anywhere people needed to hear the truth. I spoke not as a victim, but as a young woman learning to rise above stigma. I corrected myths. I educated my peers. I created space for people to ask honest questions without judgment.
Sharing my story became my strength.
Today, I lead awareness sessions for teenagers newly diagnosed with diabetes. When I look into their eyes, I see myself – the confusion, the fear, the isolation. And I tell them what I wish someone had told me at 16:
You are not broken. You are not broken. You are not broken.
You are not your blood sugar numbers.
You are not broken.
You are learning how to fight… and that alone makes you powerful.
Every time a teenager says, “I thought I was alone,” I’m reminded of why I keep speaking up. Silence breeds stigma. But when we tell our stories, we take back our power.
Why This Story Matters
This journey isn’t just about one girl living with Type 1 diabetes. It’s about how culture, silence, and misunderstanding shape our self-worth. It’s about reclaiming our narratives and using our experiences to lift others.
I’m no longer ashamed of my story.
I’m empowered by it.
And now, I use it to empower others.
Because every time a voice rises, the silence loses its strength – and the world becomes just a little kinder.
Raj Deut, Diabetes Victoria / Personal contribution
Abstract
A chance conversation at an awkward party challenged a belief I’d carried for more than twenty years with type one diabetes: the idea that I was a diabetic. That brief exchange sparked a realisation about how easily diabetes can slip from something we manage to something that defines us.
This talk explores why language matters in chronic illness and how the words we use shape identity, resilience and emotional wellbeing. Through humour and personal experience, I share how diabetes has influenced everyday life from travel to exercise, and how reframing “I’m a diabetic” to “I have diabetes” changed the way I navigated burnout, frustration and the pressure of constant self-management.
Attendees will leave with a practical, human-centred perspective on empowering language and a reminder that while diabetes affects our lives, it doesn’t have to define who we are.
Warning: video contains confronting imagery
Vinayak Rangreji, The Diabesties foundation
My name is Vinayek. I live with type 1 diabetes and visual impairment from diabetic retinopathy.
I grew up in a place where people believed children do not get diabetes. When I was finally diagnosed at seven, my parents were shocked. Instead of being offered education and support, we were surrounded by stigma. Elders said it was my karma, a punishment from a past life. My parents went from healer to healer searching for a cure. No one taught us how to actually live with type 1.
Stigma silenced our questions. In clinic visits, doctors mostly scolded us: “Why is your sugar so high? Why is your HbA1c so high?” For almost seventeen years my HbA1c stayed between 9 and 13 percent, but no one sat with us to explain what that meant or what we could change.
As a child, I didn’t even know the word “hypo”. I just said, “I am hungry.” I was given normal food, not fast sugar. When I said I was still hungry, I was labelled greedy and scolded. I learned to stop asking for help and to sneak food instead. At school and in my family, I was treated as “always sick” and too fragile to join in. I became quiet and withdrawn.
Just as I was ready to build a creative career in photography and design, diabetic retinopathy took most of my vision. Losing my sight meant losing my dreams, and I felt completely worthless.
The turning point came when I found the type 1 community and Diabesties. For the first time I felt understood, educated, and not blamed.
Now I see children with type 1 as small plants. If we water them with knowledge, acceptance and support, they can bloom. If we water them with stigma and silence, they grow up feeling like cactus. My purpose now is to help families, professionals and communities become better gardeners, so no child with type 1 must live the life I did.
Jane Speight, ACBRD
| Co-authors: | Elizabeth Holmes-Truscott; Chris Lee; Renza Scibilia; Timothy Skinner |
Background
Landmark studies of the late 1990s/2000s provided compelling evidence about the prevalence and potential to prevent/delay onset of type 2 diabetes. They led to headlines (e.g. “diabetes tsunami”, “burgeoning crisis”, “58% preventable!”) focused on public health, economic burden and personal responsibility, perpetuating diabetes stigma. These simple stories stuck, becoming the dominant diabetes narrative of the past 25 years, masking important nuance, such as selective recruitment, intensive interventions, and non-modifiable risk factors, including genetics/epigenetics, ethnicity and age.
Opportunities
We cannot ‘prevent’ our way out of diabetes or diabetes stigma, but society can support better health and healthcare for all. This requires evidence to be reported with attention to empathy and equity, with fundamental shifts in messaging: from epidemic metaphors to shared humanity; from economic burden to investment in wellbeing; from blame to collective support; and from deficit-focused ‘prevention’ to strengths-based ‘health promotion’. The latter naturally lends itself to gain-framed messaging, e.g. healthy ageing, and recognising structural barriers to optimal health, e.g. financial and food insecurity, unsafe environments.
Challenges
We live in the age of ‘click bait’. Current systems reward simplistic, blame-tinged “epidemic” stories rather than nuanced communications. If simple stories stick, we need greater care with grant proposals, research papers, media releases and campaigns, to ensure simple, stigma-free stories stick for the next 25 years.
Recommendations
Diabetes communications must embed empathy and equity as non negotiable, from research outputs to headlines. For example, media releases need to convert easily and safely into stigma-free stories, following clear language and framing policy, with key messages that authentically centre lived experience, structural determinants and supportive solutions; plus brief editorial notes on preferred terms to deter stigma-laden edits. We need explicit standards, training and accountability, otherwise empathetic and equity-focused messaging will be considered optional, and the first thing cut to create brevity or impact.
Jane Speight, ACBRD
| Co-authors: | Elizabeth Holmes-Truscott; Timothy Skinner |
Background
Diabetes research and clinical practice relies on the use appropriate assessment tools. Many validated person-reported outcome and experience measures (PROMs/PREMs) and clinical outcome assessments were developed at a time when recognition of stigma was limited. The language used in these materials can inadvertently perpetuate stigma through terms like “diabetic”, “non-compliant”, “poor control”, or deficit-focused framing. Research demonstrates that stigmatising language negatively impacts psychological wellbeing, self-management, and clinical outcomes. As understanding of person-centred care has evolved, there is growing recognition that the language in diabetes assessment tools requires systematic review and updating.
Opportunities
A comprehensive language review offers the opportunity to destigmatise diabetes research and clinical practice by identifying problematic terms, developing evidence-based alternatives that maintain measurement validity, and creating guidelines for future development of assessment tools. By engaging people with diabetes in this review process, we can ensure materials genuinely reflect their experiences and preferences. This work could establish international standards for respectful, empowering language in diabetes assessment tools.
Challenges
Challenges include maintaining psychometric properties and validity when modifying established instruments, ensuring changes do not compromise data comparability, and achieving consensus across diverse cultural and linguistic contexts. Revalidation of modified instruments requires significant resources and time. There may be resistance from researchers invested in existing tools, concerns about disrupting research protocols, and practical challenges of updating materials with multiple translations. Balancing the need for change with methodological rigour and practical feasibility requires careful navigation.
Recommendations
Such work may require:
Jane Speight, ACBRD
| Co-authors: | Elizabeth Holmes-Truscott; Timothy Skinner |
Background
The negative framing of diabetes in public campaigns and the media is a key facilitator of diabetes stigma. Such messaging often uses simplistic portrayals of diabetes, its complications, and “modifiable” risk factors, alongside urgency-invoking language (e.g., “costly” and “burgeoning” “epidemic”), to promote individual behaviour change and/or appeal to funders and policymakers. Paradoxically, this messaging may actively harm health outcomes, reduce help-seeking among those at risk or living with diabetes, and undermine policy advocacy by reinforcing diabetes stigma.
Opportunity
Evidence from social psychology demonstrates that stigma reduction requires ongoing, multi-level intervention, including responsible campaigning and reporting, as well as accountability for when harm is perpetuated. Successful stigma-reduction initiatives in other areas, e.g. mental health, have succeeded through sustained pressure on organisations and systems to drive meaningful improvements in public messaging. For example, SANE Australia’s StigmaWatch program promotes responsible reporting on mental ill-health and suicide through public monitoring and response mechanisms. The diabetes community now has both the scientific evidence and collective power to demand more sophisticated and sensitive campaigning and reporting.
Challenge
Communicators with limited time and resources may prioritise reach and media cut-through over effectiveness and ethics. Many communicators lack evidence-based guidance, as well as systematic, evidence-informed approaches to campaign development and evaluation. They also lack the accountability and improvement mechanisms required to drive meaningful and sustained change.
Recommendations
‘DiabetesStigmaWatch’ could function as a public accountability and improvement mechanism that:
Evidence from other fields confirms change happens when stigmatising approaches become too costly to maintain.
Lurina Fourie, The Glucose Glitch
Using an age-old concept, I bring diabetes awareness and education to schools and healthcare professionals in a fun, interactive way that makes the information truly stick. I’m always creating new versions of the game, and the latest edition focuses on one of the most important topics of all: how to end diabetes stigma. Video for abstract available here: https://www.youtube.com/watch?v=Pg3ntMeZYwg
Radhika Shrivastav, HRIDAY
| Co-authors: | Riddhi Modi; Amrita Rupani; Hari Chandran; Monika Arora; Mansi Chopra; Rajendra Pradeepa; Archana Sarda; Seema Srivastava; Maggie Stimpson |
Background
In India, people living with diabetes (PLWD) in marginalized communities face persistent barriers to equitable care, exacerbated by entrenched social stigma and misinformation. These stigma-related challenges delay diagnosis, restrict access to treatment, and negatively shape interactions with healthcare systems and communities. This initiative positions Lived Experience Leadership at the centre of stigma reduction efforts, aiming to co-create culturally-relevant resources and strengthen advocacy capacity of PLWD to drive systems change.
Methods
Implemented by HRIDAY; All India Institute of Medical Sciences, Delhi; Udaan; Blue Circle Diabetes Foundation and; Madras Diabetes Research Foundation, in three cities-Delhi, Aurangabad, and Chennai, the initiative is being guided by a Scientific Council alongside a Lived Experience–led Wisdom Council. Three core strategies shaped the model:
Outcomes (Achieved or Expected)
The initiative is projected to reach 2 million people, including 500,000 underserved individuals, and directly engage 1,000+ PLWD. Additional 1 million people will be reached through expanded offline and online networks. Lived Experience Ambassadors are actively advocating for meaningful PLWD involvement, equitable access to affordable care, early diagnosis, and stigma-free support systems. Early evidence shows strengthened community engagement and growing momentum for PLWD-led policy and programme dialogue.
Lessons Learned
Lived Experience Experts are uniquely positioned to lead stigma reduction through authenticity, empathy, and cultural insight. Sustainable and scalable impact requires multi-sectoral and multi-stakeholder partnerships that uphold PLWD leadership at every level. Anchoring programmes in lived experience enhances trust, strengthens advocacy, and advances equitable, person-centred diabetes care.
Description of how people with lived experience are / have been meaningfully involved
The grassroots to global initiative is powered by lived experience leadership. The initiative has been conceptualized, planned and implemented, with the guidance of nearly 200 lived experience diabetes Ambassadors from all across India. These Ambassadors have brought community voices by sharing lived experiences, co-creating awareness and educational resources, leading local engagement activities, and expanding the Diabetes Ambassador Network through peer nominations and storytelling.
Community conversations were instrumental in channelizing lived experiences, dispelling myths, and co-creating locally relevant solutions for diabetes prevention and care. The Wisdom Council, steered by people living with diabetes, provided strategic and innovative guidance to strengthen and sustain the Diabetes Ambassador Network through creative community mobilization, partnerships, advocacy, and dissemination efforts that amplify the campaign’s reach from grassroots to global levels.
Natalie Logan, Diabetes Victoria
| Co-authors: | Sab Hoskin, Jane Robinson |
Abstract
The Diabetes Camps Victoria program for 5 to 17 year olds living with type 1 diabetes has run for over 70 years.
The aims of the program are for children and adolescents to:
For parents and carers to:
Diabetes Victoria’s Camps program has supported 650 campers over the past three years. Camps run for 1 to 3 nights depending on the age group. Campers are selected prioritising those who are newly diagnosed, from disadvantaged backgrounds, and from rural and remote areas. Many children from remote areas and certain cultural backgrounds experience a high level of stigma and discrimination in their communities.
Parents have described these camps as ‘life changing’. Campers often report feeling ‘normal’ in this camp setting and feel like they are ‘not alone’ in living with their type 1 diabetes. Campers learn how to advocate for themselves within the wider community and learn from their peers about how they navigate stigma and discrimination, providing them with tools to use in their everyday life.
Shiara Pillay, Sweet Life Diabetes Community
| Co-authors: | Bridget McNulty |
Background
Diabetes is the number one killer of South Africans. So when we talk about diabetes stigma, it’s not just about the very real mental health toll, but the practical, deadly risk of pervading stigma surrounding diabetes:
Methods
In 2025, for the first time, Sweet Life launched a nationwide diabetes stigma campaign: #DiabetesLooksLikeMe.
Our landing page (https://sweetlife.org.za/diabeteslookslikeme/) and social media shared an impactful 40 second video of South Africans with diabetes saying, “Diabetes looks like me” and we invited those with and without diabetes to post a selfie on 14th May to show that diabetes can look like anyone.
A combination of lived experience stories, a strong media drive and an in-person media event that shared lived experience and a diabetes fact sheet, we began dismantling the pervasive stigma around diabetes in South Africa.
Outcomes
Please see details in attached report
Lessons Learned
There is still much work to be done. Each year will build on the previous impact – in 2026 we will include lived experience champions in all 9 provinces to further spread the message from the ground up.
Lived Experience Involvement
In every stage from ideation to content creation and interviews. Nothing was done without lived experience being present.
Leah Pascoe, Rural Doctors Network
Abstract
I have lived with Type 1 diabetes for over 20 years and coordinate a program supporting people living with Type 2 diabetes across rural and remote New South Wales, Australia. Through this dual perspective, I see how stigma affects confidence, communication and early engagement with care. Many people living with Type 2 diabetes feel judged or blamed, which contributes to silence and withdrawal from health services. Building a confident, stigma aware workforce is essential to changing this.
Through the Care Partnership Diabetes program, we developed a consumer led and consumer informed approach to diabetes workforce development. This includes a scholarship program enabling rural health professionals to complete diabetes education qualifications, structured mentoring and case management to support success, partnerships with GP practices and Aboriginal Community Controlled Health Services to strengthen local diabetes care, and service enhancement models that promote culturally safe, practical support. We also established the Western NSW Diabetes Workforce Network to reduce isolation, increase collaboration and support clinicians working in remote areas.
Lived experience guides every stage of the program, helping identify gaps that may be invisible to those without diabetes, improving communication, and ensuring stigma aware training. The scholarship program has increased workforce capability, with graduates now confidently delivering diabetes education across rural NSW. GP practices and ACCHSs report improved engagement, stronger referral pathways and better use of diabetes technology. The workforce network has strengthened peer support and created safer spaces for collaboration.
Reducing stigma in the workforce has increased confidence among people living with Type 2 diabetes to speak openly about their experiences, ask questions and seek support earlier. Being involved in this work has shown me the impact of consumer leadership and has inspired me to pursue a career in diabetes research, beginning with an undergraduate degree in Health Science in 2026.
Matthew Larsen, Diabetes Action Canada/ University Health Network
| Co-authors: | Al Martin; Ian Patton; Linxi Mytkolli |
Background / Aim(s)
People with type 2 diabetes who live in larger bodies often describe clinical encounters where their concerns are reduced to “diet and exercise,” regardless of history or context. These interactions can feel shaming, erase effort and delay appropriate care. As part of the Diabetes Action Canada Research-to-Action Fellowship, in partnership with Obesity Canada, this project aims to model what it looks like to “flip the script” on weight and diabetes stigma using short, scenario-based comics.
Methods (who, what, where)
Two Fellows with lived experience of type 2 diabetes (also living with obesity) led a virtual co-design session with approximately 14 people with lived and loved experience of type 1 and type 2 diabetes, obesity, homelessness and other intersecting conditions. Participants shared real stories of stigmatizing clinic visits and brainstormed what supportive interactions could sound like instead.
These insights, combined with Obesity Canada’s weight-bias guidance, informed two “Flipped Scripts” comics. Each comic shows a common harmful encounter (for example, being handed generic diet advice after decades of effort, or being shamed about weight minutes before surgery) followed by a “flip” that centres respect, consent and concrete support. The comics are available as free digital panels and printable posters with a QR code linking to more information.
Outcomes (achieved or expected)
Early use in Obesity Canada and Diabetes Action Canada workshops suggests the comics quickly spark discussion, help providers recognise themselves in the “before” scenes and offer concrete language for doing better. Expected outcomes include increased reflection on weight bias, more patient-centred communication and wider use of the comics in training, clinic waiting rooms and community education.
Lessons Learned (for scaling / adaptation)
Using comics to pair “harmful script” and “flipped script” makes abstract concepts like stigma and weight bias visible and practical. Scenario-based dialogue gives providers a starting point for change instead of only telling them what not to say. The format is easily adapted to other clinical settings and communities by co-creating new scenes and scripts.
Description of how people with lived experience are / have been meaningfully involved
The project is co-led by two Fellows with type 2 diabetes, one also living with obesity, whose experiences shaped the core scenarios and tone. The focus group of about 14 participants with lived experience of diabetes, obesity, homelessness and other marginalisation informed every stage—from selecting situations that felt most harmful to choosing the words that felt respectful in the “flipped” panels. All contributors were compensated, and their stories remain at the heart of the final comics.
Anmol Budhiraja, Diabetes Action Canada (DAC)
| Co-authors: | Jeremy Auger |
Background / Aim(s)
This project is part of the Diabetes Action Canada Research-to-Action Fellowship in partnership with the Indigenous Diabetes Health Circle (IDHC). Community members described being misdiagnosed, having tests delayed and feeling dismissed in appointments—experiences that disproportionately affect Indigenous, Black and Brown people. Our aim is to create practical, culturally grounded tools that help people recognise symptoms, ask for essential tests and assert their rights in clinical settings.
Methods
Together with IDHC, we held a co-design session with over two dozen Indigenous, Black and Brown participants who had lived or loved experience of diabetes or had supported family through misdiagnosis. Sharing Circles explored how racism, weight stigma and stereotypes about “who gets diabetes” shaped care and silenced questions.
Using participants’ words, we drafted “Diabetes Answers for Us” wallet cards listing common symptoms, key tests and plain-language rights for medical appointments. A short follow-up survey invites wider feedback and offers people the chance to review drafts before finalisation.
Outcomes (achieved or expected)
The wallet cards and a companion easy-to-read guide will be freely available through Diabetes Action Canada and IDHC in early 2026. We expect them to provide discreet, portable support that increases confidence to ask for tests, helps people connect symptoms to diabetes and enables them to challenge biased or dismissive care in real time.
Lessons Learned (for scaling / adaptation)
Co-design confirmed that shame around diabetes and misdiagnosis is cultural and systemic, not personal. Low-barrier tools like wallet cards can interrupt that shame by giving people accessible language and questions. Grounding the tools in Indigenous, Black and Brown voices, plain language and low-tech design offers a model for adapting this work to other racialized and diaspora communities, including future versions for India.
Description of how people with lived experience are / have been meaningfully involved
The project is led by two Fellows whose lived, loved, learned and laboured experience spans type 1 diabetes, a new type 2 diagnosis, Indigenous identity, Indian diaspora identity, family caregiving and chronic-disease work. The co-design session with more than two dozen community members shaped every stage—from identifying systemic barriers and emotional triggers to deciding which rights, symptoms and tests to include. Their insights continue to guide the wording, visuals and evaluation of the final tools, ensuring they reflect real needs and restore agency in care.
Jyotsana Rangeen, Diabetes India Youth in Action
Abstract
DiaBeatStigma began as a social media initiative to confront the silence, shame and misunderstanding surrounding diabetes, particularly among women in India. Having seen how stigma leads to isolation, delayed care and emotional distress, I created a space where women could learn the art of living well with diabetes, free from judgment.
Through posts, reels, lived-experience narratives and myth-busting content, the platform shares real stories that humanise diabetes and challenge the stereotypes that often label women as “careless,” “responsible for their condition,” or “unfit” for societal expectations. As the community grew, DiaBeatStigma expanded beyond awareness into action. I conducted interactive online sessions, facilitated one-to-one counselling, and organised camps encouraging women to reclaim their confidence, speak openly about their health, and support one another.
These stories and conversations reveal the everyday impact of stigma, being blamed for food choices, judged for insulin use, or discouraged from seeking care. They also highlight resilience: women finding strength in peer support, making informed decisions, and advocating for themselves within families, workplaces and the healthcare system.
DiaBeatStigma continues to amplify lived experience, foster connection, and inspire change. Its purpose is simple yet powerful: to show that diabetes is not a personal failure, and women deserve dignity, understanding and equal access to care.
Women living with diabetes have shaped every aspect of the project. Their stories, interviews, daily challenges and successes form the core content. Many participants contribute anonymously or openly, share testimonials during sessions, and provide feedback. Their lived experience is the foundation of DiaBeatStigma’s message and impact.
Deanne Minniecon, Diabetes Australia
| Co-authors: | Fleur Kelly, Grace Ward, Elizabeth Holmes-Truscott |
Background
Diabetes stigma negatively affects health, undermines self-care, and creates barriers to accessing education and support. For Aboriginal and Torres Strait Islander peoples, experiences of blame and shame are interrelated with the ongoing impacts of colonisation, structural disadvantage, and racism within Australian. Aboriginal and Torres Strait Islander health workers are well placed to recognise and address diabetes stigma within their communities.
Methods
The National Diabetes Services Scheme (NDSS), in collaboration with an Aboriginal and Torres Strait Islander expert reference group, the Australian Diabetes Educators Association, Diabetes Australia, and the Australian Centre for Behavioural Research in Diabetes, developed a brief online learning module that provides a culturally grounded perspective on diabetes stigma and discrimination.
Outcomes
The freely available module highlights the unique experiences of Aboriginal and Torres Strait Islander peoples and equips health professionals with the knowledge and practical strategies to recognise and reduce diabetes stigma and promote culturally safe care. To complement the training, culturally relevant collateral was developed under the message “Talk good ways – no more shame”, encouraging respectful language and reducing shame in conversations about diabetes amongst Aboriginal and Torres Strait Islander people. These resources can be displayed in clinics and community spaces. Since launch in September 2025, 59 individuals have completed the training and 16 are currently in progress as of end of November 2025.
Lessons Learned
Lived-experience–led storytelling in local languages powerfully challenges stigma, builds trust, and creates community ownership. Partnerships between HCPs and T1D advocates ensure emotionally resonant, clinically accurate messages. For scaling, adaptable toolkits, multilingual digital content, and collaborations with schools, workplaces, and health systems are key.
Meaningful Involvement
Module development required navigating limited empirical evidence specific to diabetes stigma in Aboriginal and Torres Strait Islander communities, while drawing on strong community expertise and broader literature. Effective partnership work relied on Aboriginal and Torres Strait Islander co-leadership and shared decision-making. Establishing mechanisms for ongoing evaluation will support refinement and build the evidence base. This initiative promotes awareness and action to reduce diabetes stigma, fostering inclusive and respectful care for Aboriginal and Torres Strait Islander peoples with diabetes.
Danica Collins, Dia-Log: The Insulin for Your Soul
Abstract
Traditional diabetes education teaches people how to manage glucose and insulin, yet rarely addresses the emotional, behavioral, cultural, and identity-based realities that shape daily life with diabetes. For the first ten years of my diagnosis, I navigated diabetes entirely alone. I was told I had the “rich white person’s disease,” that I was “too skinny” to be diabetic, and that my scarring “wasn’t real.” I lacked community, whole-person guidance, and access to tools that reflected my experiences as an African American woman. What changed my trajectory was the moment people began asking how I was living well — how I traveled, exercised, handled decision fatigue, advocated for myself, and built a life that did not feel limited by diabetes. Their questions revealed a widespread unmet need. I became a coach because others saw something in my thriving that they wanted for themselves. I needed this support first, and then expanded it for the community, now working with health systems and organizations globally to integrate wellness coaching into their care models.
In response to this need, I created The Daily Drop in 2023 — a holistic reflection framework that helps individuals move from managing diabetes to living and thriving with it. The Daily Drop shifts focus from numbers to the real-world factors that influence diabetes: emotional wellbeing, stress, identity, finances, fatigue, sleep, relationships, habits, and community. It incorporates on-brand “Daily Drops,” simple evidence-based behavioral practices that support stability, awareness, advocacy, and resilience. The framework is delivered through digital education, community sessions, global coaching, and wellness advocacy. It is intentionally accessible regardless of location, insurance status, or technology access.
Since its introduction, The Daily Drop has reached more than 10,000 people worldwide. Participants consistently shared that they knew how to manage diabetes, but no one had taught them how to actually live with it. A common theme was realizing that emotional triggers, loneliness, financial pressure, disrupted sleep, and daily habits were influencing their blood sugar as much as food or insulin. Many reported reduced shame, improved emotional regulation, stronger self-advocacy, and clarity when navigating diabetes technology that may not have been affordable, accessible, or right for their bodies. Community engagement further decreased isolation and validated lived experience across cultures.
This work demonstrates that diabetes stigma is experienced differently across intersections of race, body size, culture, and access, yet the common thread is a lack of whole-person support. Diabetes does not have to be limiting, and a diagnosis is not an ending. When individuals understand their habits, emotions, needs, and sources of support, they gain the ability to live their healthiest lives and truly thrive with diabetes. By centering daily habits, emotional literacy, and community connection, The Daily Drop reduces stigma at its roots and helps individuals build a life where thriving becomes possible.
Lea Leleta, DiabetNO1
Abstract
In Bosnia and Herzegovina (BiH), discussions about T1D remain limited, especially in rural areas where stigma and misinformation persist. Children with T1D often lack tools that help them communicate their experiences in an empathetic, age-appropriate way to peers and educators. Early research showed no children’s book in the region addressing diabetes through storytelling and emotional learning. To fill this gap, I created Lea and Her Diabetes the first children’s illustrated book on T1D in BiH, aiming to strengthen empathy, understanding and supportive environments.
The project used a child-centered visual design approach, applying key principles of design, color, typography, hierarchy and visual harmony to guide illustration and layout. Content focused on emotions and empathy rather than medical instruction, helping children relate to feelings such as sadness, frustration and resilience. Based on color-psychology research, I developed a cohesive palette that is calm and keeps children’s attention. The book includes peer support, such as a classmate noticing symptoms and offering help, reinforcing open communication. Typography choices, rounded, highly legible fonts and larger sizes supported early readers. Feedback was gathered from children with T1D, parents, peers, teachers and diabetes associations in urban and rural settings.
Children with T1D identified strongly with the main character, making it easier to explain diabetes to peers and teachers. Parents reported that their children felt understood and more willing to talk about diabetes in school and with friends. Children without T1D showed curiosity and empathy, engaging with the story. Kindergartens, primary schools, high schools, and educators requested copies for libraries and educational activities.
In communities with limited access to diabetes technology, low-cost design-based interventions can still make meaningful impact. Early childhood is a critical stage for breaking stigma, and interest from children without T1D highlights the power of empathy-based storytelling. The project shows potential for adaptation in other regions.
Riddhi Modi, Empower T1D
| Co-authors: | Manisha Gupta; Rutul Gokalani; Amit Kumar Dey |
Background
People with Type 1 Diabetes (T1D) feel judged or unsafe injecting insulin in public, leading to missed doses, secrecy, and distress. #InjectAnywhere is a community-led movement by Empower T1D to end the stigma of insulin administration outside the home—at schools, workplaces, and public spaces—and to build confidence and safety for people on insulin therapy for better outcomes.
Methods
The initiative brings together healthcare professionals and T1D community to co-design awareness campaigns, walkathons, workshops, and digital content across India. Activities include stigma-focused education sessions in schools and clinics, social-media campaigns in multiple regional languages, short educational videos, and toolkits for teachers, employers, and community. People with Type 1 Diabetes (T1D) contribute photos, stories, and messages in their own languages, and local T1D support groups collaborate to host events in different states.
Outcomes
The campaign has mobilized walkathons and awareness drives with participation from T1D communities, caregivers, and clinicians, reaching audiences in diverse regions and languages. Participants report feeling more comfortable discussing and taking insulin in public, with organizers observing normalized conversations among children and peers. Early impacts include improved glycemic control, better HbA1c levels, increased Time in Range (TIR), and enhanced quality of life (QoL) due to consistent insulin adherence. The movement is expanding across clinics, schools, and online platforms, with growing pools of user-generated stories and visual content to strengthen advocacy.
Lessons Learned
Lived-experience–led storytelling in local languages powerfully challenges stigma, builds trust, and creates community ownership. Partnerships between HCPs and T1D advocates ensure emotionally resonant, clinically accurate messages. For scaling, adaptable toolkits, multilingual digital content, and collaborations with schools, workplaces, and health systems are key.
Meaningful Involvement
People living with T1D shape campaign messages, lead events, and act as visible role models, making #InjectAnywhere a movement designed with and for the community to alleviate stigma.
Riddhi Modi, UDAAN
| Co-authors: | Kamlesh Chitte, Manjusha Barve |
Background
In low-resource settings, Type 1 Diabetes (T1D) stigma commonly begins at the earliest point of contact: the rural doctor who frames insulin as frightening, the pharmacist who reinforces misconceptions, and the school that restricts participation due to hypoglycaemia fears. These three influencers shape community beliefs, creating a cascade of fear, secrecy, and delayed care.
TARA (Type 1 Advocacy for Rural Awareness) is a structured, low-cost, youth-led model designed to interrupt this stigma pathway at its source by finding their voice through community empowerment and offer a replicable global solution.
Methods
30 youth with T1D from 12 districts were trained through a standardised curriculum centred on stigma recognition, counter-narrative building, ethical storytelling, and behaviour-change communication. Each advocate received a replicable toolkit including: high-visibility posters (“Young people can do everything with insulin”), youth testimonial videos, myth–fact cards, pre/post questionnaires, and stigma-mapping sheets.
The intervention followed a structured seven-step operational cycle, whereby each advocate went back to work in their own respective district. Diagram attached.
Outcomes
Across 144 villages, advocates engaged 5580 teachers/students, 122 pharmacists, and 109 rural doctors. Questionnaire analysis showed clear improvement in supportive behaviour among all three influencer groups. Poster visibility remained high, testimonial videos reached 25000+ people in the last 5 months. Advocates themselves reported reduced self-stigma and increased recognition as reliable “resource persons” within their communities.
Lessons Learned
Effective stigma reduction in low-resource settings requires shifting attitudes among the earliest influencers—doctors, pharmacists, and schools—supported by youth leadership, visible messaging, and lived-experience narratives. These create culturally sensitive and sustainable changes. TARA demonstrates a globally adaptable, low-cost model capable of producing rapid, sustainable shifts in community beliefs and healthcare behaviour.
Elizabeth Holmes-Truscott, ACBRD, Diabetes Victoria and Deakin University
| Co-authors: | Emmanuel Ekpor; Eloise Litterbach; Renza Scibilia; Partha Karr; Jane Dickinson; Susan Guzman; Matthew Garza; Mariam Asaad; Mark Barone; Chitra Selvan; Tejal Lathia; Jazz Sethi; Amy McInerney; Peter Senior; Timothy Skinner; Jane Speight |
Background
Language shapes how diabetes is perceived and experienced. Since the first national position statement was published (Australia, 2011), numerous (inter)national statements and related resources have emerged. To date, there has been no synthesis of their development, scope, adoption and implementation.
Methods
This impact review, conducted by a multidisciplinary team including people with lived experience, mapped the evolution of diabetes language statements and resources. Relevant documents were identified via citation searches and websites (LanguageMattersDiabetes.com; dStigmatize.org), and examined for development processes, target audience, scope, and content. Evidence of adoption was sourced from peer-reviewed literature.
Outcomes
Twenty-seven documents were identified, from 18 countries and two multi-country statements. Most were published as the official position or consensus statements of diabetes organisations, developed by invited professional and lived experience experts. Most involved translation or adaptation of earlier guidance. While statements are assumed to reflect theory, evidence and community perspectives, few explicitly describe structured mechanisms for community input. While most do not specify diabetes types or settings, six are specific to diabetes subgroups, six are tailored to healthcare and one to media reporting. Of the 50+ terms identified as problematic, around half were not in the original 2011 statement, reflecting evolving recognition of negatively-experienced language. Most statements articulate core communication principles: person-centred, strengths-based, empathetic, and non-judgemental. Evidence of adoption is apparent, with increasing integration into clinical standards, professional training, conference and journal policies. Gradual shifts in language have been observed in some research and media contexts. However, implementation remains uneven, and stigmatising language persists across settings.
Lessons Learned
The #LanguageMatters movement is gaining traction, yet empirical evidence on community preferences and rigorous evaluation of adoption remain limited. Language is evolving with increasing awareness and emerging technologies, screening, and therapeutics. Further outcomes-driven research, policy-level implementation, and context-specific strategies are needed to support stigma-free communication across settings.
Benjamin Olorunfemi, Rays of Hope Support Initiative (ROHSI)
Abstract
Growing up in Nigeria, I witnessed firsthand the devastating impact of diabetes-associated stigma. My uncle’s experience with type 2 diabetes was shrouded in fear, misinformation, and isolation. The misconception that diabetes is contagious led to his social exclusion and, ultimately, his untimely death.
In Nigeria, diabetes carries a heavy social and cultural burden, rooted in beliefs of spiritual affliction or personal failure. This stigma forces people to hide their condition, delay treatment, and suffer in silence, leading to complications and premature mortality.
Through my organisation, I have developed a grassroots model that fosters connection and education. A dedicated WhatsApp platform has created a safe space for people living with diabetes to share experiences, find support, and break isolation. One community member, who had hid his condition for years before joining our community due to shame, finally found understanding and accepted care through our community
Our work demonstrates that community support, education, and practical aid can empower individuals to “live and make a life out of diabetes.” To end stigma, we must advocate for a fundamental shift in how interventions are designed. People living with diabetes must have a seat at the policy-making table.
Ernest Groenewald, SA Diabetes Advocacy
Growing up with type 1 diabetes in South Africa meant learning to manage not only a complex medical condition but also the stigma that followed it. I was diagnosed at six years old in a public hospital in KwaZulu-Natal, and from the very beginning, my condition changed the way people treated me. Teachers saw me as fragile, other children avoided me as if I were contagious, and I was often excluded from school activities and friendships. Instead of being seen as a child who needed support, I felt like a burden that needed to be managed.
As a “brittle diabetic,” I spent much of my childhood in hospital wards rather than classrooms. Over the years, I developed complications, including chronic kidney disease, diabetic neuropathy, and diabetic retinopathy. I was also recently diagnosed with celiac disease. These additional conditions intensified the misunderstanding and judgement I faced—many people assumed my complications were the result of poor management, rather than the reality of living with a relentless and unpredictable autoimmune condition.
Despite everything, stigma became the fire that pushed me into advocacy. I wanted to speak up not only for myself but also for the many young South Africans who feel unseen, misunderstood, or blamed for their condition. In the past, I was involved with Diabetes South Africa in Port Elizabeth and served as the Camp Director for Camp Diabetable. Although I have stepped away from that role, my commitment to advocacy has only grown. Today, I’m focusing my energy on access, empowerment, and stigma reduction through #insulin4all and T1International.
Through this presentation, I hope to bring a South African lived-experience perspective to the global conversation on diabetes stigma.
Dr. Vanshika Aggarwal, Alignia Foundation
| Co-authors: | Deeksha Dev |
Background
Young adults (18–35 years) living with diabetes in India often manage their condition while navigating major life transitions; university, early career roles, financial independence, and relationships. Despite these pressures, diabetes care in India remains primarily biomedical, leaving limited space for emotional experiences such as fear, burnout, shame, or uncertainty. Through counselling sessions and digital conversations, Alignia observes that many young people feel unprepared for the psychological demands of daily management, especially when support systems do not recognise mental health as part of diabetes care.
Challenges
Young adults report privately managing anxiety about fluctuations, fear of judgement, and pressure to appear “disciplined” in front of clinicians. Many described forging or selectively adjusting logbook entries, downplaying highs and lows, or lying about food habits to avoid criticism. Some reported presenting an “ideal patient version” of themselves during consultations, suppressing questions or emotional distress to appear competent. Others hid injections, alarms, or symptoms in academic and work settings to avoid being judged as unreliable. These behaviours reflect not dishonesty, but a lack of emotional safety in care environments where psychological needs are overlooked.
Recommendations
Drawing from Alignia’s mental health practice with young adults, three feasible steps emerge:
Recommendations
Young adults are motivated to engage in care, but they need emotional infrastructure that acknowledges the weight of daily management. When mental health support becomes part of diabetes care, confidence, agency, and continuity improve.
Dr. Vanshika Aggarwal, Alignia Foundation
Abstract
This storytelling contribution shares my lived experience of being diagnosed with type 1 diabetes at seven years old in a small town in northern India, where awareness and resources for children living with diabetes were extremely limited. My diagnosis introduced my family and me to multiple layers of stigma: cultural beliefs linking illness with blame, societal assumptions about capability and future prospects, and the internal doubt that grows when a child repeatedly hears that they are defined by a condition.
My family responded with resilience. With no specialist care or accessible education, my mother sought printed research articles and became my first educator. My father and brother formed a circle of emotional and practical support. Despite this, stigma from the community; including misconceptions about responsibility, marriage, and physical ability shaped many of my early experiences. Over time, this contributed to self-stigma that influenced how I engaged with my own care during adolescence.
A severe medical crisis in 2019 became the turning point that transformed denial into responsibility and silence into voice. This experience guided me into healthcare, advocacy, and later into global health studies, where I recognised how cultural context and systemic inequities shape the lives of people living with diabetes. Today, I work in public health programmes across underserved communities while working for a foundation focused on integrating mental health into chronic illness care.
The creative medium of this contribution is a narrative oral presentation. It traces a path from cultural misunderstanding to self-empowerment, illustrating how stigma operates across personal, social, and structural levels and how support, representation, and community can counter it. My aim is to contribute a perspective that highlights the emotional realities of diabetes stigma and the transformative potential of lived experience in reshaping care and creating belonging.
Deeksha Dev, Alignia Wellness Foundation
| Co-authors: | Dr. Vanshika Aggarwal; Dr. Jyoti Seth; Dr. Firdous Shaikh; Dr. Srishti Puri |
Background / Context
In India, diabetes is interpreted not only as health condition but also as a marker of capability, desirability and future security. When diabetes can be managed quietly with tablets, stigma stays hidden. Visible care such as insulin injections makes the condition socially “real”, triggering judgement shaped by gender. Women are expected to protect the family reputation and reproductive futures, while men are expected to remain physically strong and financially reliable. These challenges significantly affect social well-being.
Challenges
Women describe being encouraged to conceal their diagnosis or hide injections during marriage negotiations to avoid being deemed unfit for marriage or motherhood. Family gatekeeping of food, mobility, and appointments is common, framed as “protecting fertility,” but it often reduces autonomy. Women fear being blamed for “passing the condition to a future child.” At work, capability is questioned due to assumptions about stress tolerance and productivity, increasing economic dependence.
Men reveal different pressures: hiding emotional distress to appear strong, avoiding visible care to maintain confidence from colleagues, and experiencing judgement around stamina, body changes, or sexualhealth concerns. Concerns about job security and credibility lead to delayed disclosure and supportseeking. Across genders, stigma drives silence, selfblame, and reduced engagement with care.
Recommendations
Reflections
Stigma shapes how people live with diabetes long before they seek medical care. When judgement is replaced with dignity and supportive dialogue, individuals gain emotional safety and confidence in their diabetes journey.
Meet Shinde, P.N.Doshi women’s college – S.N.D.T University
| Co-authors: | Sayli Jadhav, Chitra Selvan, Tejal Lathia |
Abstract
In the last decade multiple researchers across biomedical and social sciences – particularly anthropology, sociology and psychology – have explicated the linkages between stigma experienced by people living with Type 2 diabetes and their bio-psycho-social wellbeing. There is also compelling evidence connecting subjective experiences of stigma with fluctuations in active self-management of blood sugars. Owing to largely quantitative research populating the academic terrain; the conceptual and experiential particularities of what accounts for stigma, remains implicit in the context of people living with diabetes. While most researchers use the term stigma, they seldom theoretically ground or operationally define the term, thereby assuming a consensus about what it means across cultural specificities. Against this background the authors* of the current paper aims to theorize the nature and scope of the psychosocial experience of stigma as a conceptual category. It starts by explaining how stigma has been defined and theorized across disciplines, models and frameworks followed by delineating the overlap and differences between stigma, prejudice and discrimination. It then argues for the necessity and utility for a separate conceptual category of diabetes stigma and outlines its features using Walker and Avant’s concept analysis. The researchers propound that the resultant conceptualization of stigma would shape future theoretical and empirical work by refining its approach to measurement, and intervention within the field of diabetes care and management.
(* one of the authors on this paper is a person living with Diabetes, and two other authors are medical practitioners working with persons living with T2DM.)
Mark Erwin
| Co-authors: | Ian Litterbach; Eloise Litterbach |
Background / Context
Many people assume the hardest part of being a firefighter is facing trauma, death, and destruction. An equally significant yet invisible challenge, is the stigma and ambiguity of having diabetes in the Fire Service.
Opportunities
Firefighting demands resilience, courage, and commitment—qualities that people living with diabetes demonstrate every day. Being a firefighter brings pride and joy to hundreds of Australian men and women, who grew up wishing to become a Firefighter, and now dedicate their lives to helping community during the worst moments of their lives.
Challenges
Having diabetes in the Fire Service can be perceived as a weakness or liability. There are major barriers for those with diabetes who aspire to join and little clarity about whether diabetes disqualifies candidates. Currently, in Australia ‘specific medical advice is only provided at the pre-employment medical stage’, after completing a highly competitive and lengthy recruitment process. For someone with diabetes requiring insulin, this could mean investing months of time and emotional effort only to be deemed “an unacceptably high risk”. This uncertainty alone discourages many from applying. Some firefighters who receive a diabetes diagnosis once in the Fire Service, will never disclose their condition, for fear of being taken off duty, and losing the career they’ve dedicated their lives to. Access to information regarding whether a person may remain employed with the Fire Service after a diabetes diagnosis is limited. This anxiety and non-disclosure may result in firefighters not seeking critical medical monitoring for health risks unique to firefighters.
Recommendations
To end diabetes stigma within the Fire Service, clarity and consistency regarding the medical criteria for people with diabetes is critical. Furthermore, transparency around medical criteria before embarking on the competitive recruitment process will allow people with diabetes to make informed decisions around seeking a career in the Fire Service.
Meaningful Involvement of Lived Experience of Diabetes:
This perspective piece was led by an individual who has been living with type 2 diabetes for three years, and who works in the Australian Fire Service. All authors have loved experience of T1D, T2D, GDM and or rarer types of diabetes.
Timothy Skinner, Deakin University
Background / Context
There is a growing body of research that demonstrate the negative impact of the language health care professionals use on people with diabetes. There is also growing body of research highlighting the stigmatising behaviour and language of health professionals, media and wider community, that results in discrimination and prejudice against people with diabetes. To date we have relied on position statements and pledges to shape and influence change in people’s language and behaviour. These approaches whilst having benefit, are slow to impact substantially in day-to-day practice. We need to engage more strategies and approaches to drive change in people, organisations and systems. Publication of consumer ratings maybe one tool to achieve this end, with a view to Naming and Faming.
Opportunities
We are familiar with the publication of consumer ratings in diverse contexts, such as online purchasing platforms lie ebay, Airbnb. The publication of consumer ratings of health professionals through sites such Healthgrades, RateMDs and health service organisations are being used by individuals to inform who and where people going for their health care. Can these same tools being used to drive quality improvement in the language used, stigmatising behaviour and discriminatory practices of health care professionals and health care organisations.
Challenges
For this to work, we need to develop appropriate rating tools that can be used across contexts, cultures and languages. This will require collaboration between consumers, health professionals and researchers to develop consumer rating that drive positive responses and changes from those being rated.
Recommendations
We should develop a platform for consumers to rate their health care professionals and organisations for their language, policies and communications. We should ask the organisations and individuals who have taken the pledge to remove stigma, to be sign up to be rated on the platform
Jane Speight, ACBRD
| Co-authors: | Elizabeth Holmes-Truscott; Timothy Skinner; Michael Vallis |
Background
Diabetes stigma remains a pervasive yet poorly quantified barrier to effective healthcare, self-management and quality of life. While clinical outcomes are routinely measured at population levels, there is no structural, multi-country approach to tracking diabetes stigma, support and inclusivity. Successful precedents exist. For example, the Social Progress Index measures societal advancement through dimensions such as personal rights and opportunity, while the New Economics Foundation uses the Happy Planet Index to evaluate countries by how efficiently they deliver long, happy lives for their residents using our limited environmental resources. These frameworks show that complex social phenomena can be benchmarked systematically and successfully when appropriate methods are applied.
Opportunities
A diabetes stigma benchmark could transform advocacy and policy by making the invisible visible. Composite indices could integrate quantitative measures (e.g. employment discrimination rates, healthcare access disparities, media representation analysis) with qualitative indicators (lived experiences, community attitudes). International comparisons could identify best practices and hold countries accountable. Time series data could enable monitoring of progress and the effectiveness of interventions. Such benchmarking could also elevate stigma reduction as a core diabetes care quality metric.
Challenges
Diabetes stigma manifests differently across diabetes types, cultures and countries, complicating unified measurement. Self-reported stigma may underestimate internalised shame, while objective measures may miss subtle discrimination. Establishing causality between interventions and stigma reduction requires longitudinal investment. Resistance may emerge when benchmarking reveals systemic failures. This initiative requires substantial resourcing.
Recommendations
We need to:
James Elliott, Voices in Action: PLWD in Global Health
| Co-authors: | Lucía Allonca |
Background
Both people living with HIV and people living with diabetes experience stigmatization and discrimination. Are there differences in how stigma and discrimination manifest against these groups? Has the stigmatization of these conditions evolved, and if so, how? What can both communities learn from each other vis-à-vis our fights for human rights and against stigmatization? It is also critical to consider intersectionality, particularly within the LGBTQ+ community, where belonging to the community itself can be stigmatizing.
In people living with diabetes, and even more so in those living with both diabetes and HIV, these can constitute multiple layers of stigma that significantly hinder access to care. This burden is especially pronounced for women within the LGBTQ+ community, including lesbian, bisexual, and trans women, who face additional barriers related to gender, sexuality, and social marginalization. This workshop will aim to address these questions.
Opportunities
The diabetes community has admired the achievements of the HIV community in shifting the narrative in ways that we would like to see ourselves. From the past focus on “lifestyle” and “it’s better to prevent than treat,” it would seem from a distance that the HIV community has achieved wins that the global diabetes community has yet to achieve at scale. Yet, is this actually the case?
Challenges
Although there are similarities in living with HIV and with diabetes, such as the lifelong nature of the conditions and the need for continuous treatment, there are also key differences. In addition, the gains achieved by the HIV community at the global level have been recently eroded, such as the scheduled closure of UNAIDS and pullbacks in funding for treatment and prevention. For LGBTQ+ individuals, especially women, these challenges are compounded by intersecting stigmas that can further limit access to care and social support.
Recommendations
This workshop will aim to land on a series of recommendations for attendees on what lessons to learn—and not to learn—from our colleagues living with HIV, taking into account the intersectional experiences of LGBTQ+ communities and the compounded stigma faced by women living with both diabetes and HIV. Perspectives of HIV+ people will be sought directly, through key informant interviews, video and scoping review.
James Elliott, Voices in Action: PLWD in Global Health
| Co-authors: | Lucía Allonca |
Abstract
Diabetes is one of the world’s most common Non-Communicable Diseases (NCDs). The term “NCDs” is a very broad grouping of conditions that also includes cancer, cardiovascular disease, oral health and many other health conditions. In today’s complex global health landscape, the positioning of diabetes within the broader NCD agenda raises important questions and tensions. Even within the category of ‘diabetes’ the differences between types are tremendous. This segment will examine the pros and cons of diabetes inclusion in the NCD agenda.
On the one hand, inclusion and association of diabetes with the NCD agenda brings clear advantages, such as increased visibility, shared advocacy platforms, and potential access to pooled resources. It allows for diabetes to be included in High-Level Meetings, such as the recent 4th High Level Meeting on NCDs and Mental Health.
On the other hand, the association with diabetes carries downsides and risks. By inclusion in such a broad category, it dilutes the unique needs of people living with diabetes and our realities. The NCD agenda is also widely understood to be one of preventable and behavioral linked diseases, which does not fit the realities of many forms of diabetes. It also carries risks: the unique needs of people living with diabetes—alongside stigma and misconceptions about the condition—may be overshadowed, and competition for limited funding could exacerbate inequities.
This debate explores both sides of the issue through a dynamic and participatory format. Participants will examine whether diabetes should maintain its own dedicated agenda to safeguard its priorities, or continue within a collaborative NCD framework to ensure political unity and resource access. The discussion will engage diverse perspectives, including those with lived experience of diabetes, and will actively encourage critical thinking, dialogue, and the co-creation of intermediate conclusions that can guide future advocacy and policy strategies.
Format: Interactive debate with structured pros and cons discussions, followed by facilitated group reflection to generate actionable insights.
Objectives:
Highlight the benefits and limitations of diabetes’ inclusion in the NCD agenda, including the risks for amplifying stigma.
Foster a participatory environment for exchanging ideas and experiences.
Reach consensus on intermediate conclusions to inform advocacy and policy decisions.
Involvement of Lived Experience: The debate will actively include people living with diabetes, ensuring their insights and priorities shape the conversation.
Stephen (Mark) Tiller, Dedoc
Abstract
No-one, absolutely no-one, chooses to have diabetes.
One of the things I learnt when studying Neurolinguistic Programming (NLP) was the concept that behind every decision is a positive intention. Which can also be restated as nobody deliberately makes a bad decision. Which means that everybody is doing the best they can at the time with the knowledge, experience and resources they have available to them.
While, in the future, they might look back with more knowledge and experience and wish they had made different choices, at the time, they were making absolutely the best decisions they could.
So, blaming someone who is doing the best they can at the and stigmatizing them is ignorant, cruel and counter-productive.
You fight stigma with good information, so if someone says something incorrect about Diabetes, educate them, and remember nobody, absolutely nobody, chooses to have diabetes.
Timothy Skinner, Deakin University
| Co-authors: | Jane Speight; Elizabeth Holmes-Truscott |
Background / Context
Recent clinical research suggests that type 2 diabetes is probably not a single homogenous condition. The identification of subtypes may have value in supporting tailored risk assessment and management approaches. Several investigators suggest between 3 and 7 subtypes of type 2 diabetes, using various methodologies with diverse clinical populations. The terminology used for these new subtypes ranges from possibly neutral labels (e.g. Type 2A, Type 2N etc) to labels that may perpetuate or exacerbate diabetes stigma and discrimination by reinforcing social narrative surrounding diabetes and corroborating intersectional stigmas (e.g. severe diabetes, mild diabetes,-obesity-related, age-related).
Opportunities
Reconceptualising diagnostic labels provides an opportunity to engage with people with lived experience of type 2 diabetes, to ensure that the new labels and terminologies used do not increase stigmatisation and, unwittingly, create increasingly marginalised or stigmatised sub-groups.
Challenges
Clinical and/or laboratory-based researchers do not appear to see the potential negative impact on the community of the “technical” language they use to describe so-called “diagnostic” sub-categories of diabetes. Similarly, journal editors may struggle to follow current recommendations for appropriate language to use when communicating about diabetes, due to evolving terms generating controversy that may not appear to be covered adequately by such guidance.
Recommendations
At present, there appears to have been no input of people with lived experience of diabetes into the labels being offered for the new sub-types of type 2 diabetes. We recommend that the clinicians, researchers and professional bodies developing clinical guidelines and terminology undertake meaningful consultation with individuals with lived experience of type 2 diabetes to develop consensus on appropriate non-stigmatising, accurate terminology for the sub-types of type 2 diabetes; and engage the wider community with lived experience of other types of diabetes to minimise unintended consequences.
Involvement of Lived Experience
This perspective is authored by professional experts in clinical psychology and behavioural diabetes research. Authors also bring lived experience of gestational diabetes, elevated type 2 diabetes risk, and loved experience of people with various types of diabetes, including type 2 diabetes.
Eloise Litterbach, Deakin University, ACBRD
| Co-authors: | Joanne Jordan; Laura Klinker; Renza Scibilia; Virginia Hagger; Uffe Søholm; Timothy Skinner; Jane Speight; Elizabeth Holmes-Truscott |
Background/Aims
Extensive evidence demonstrates the prevalence and impact of diabetes stigma, yet few interventions exist to address it. Interventions must be developed in partnership with community to ensure they are relevant, acceptable and do no harm. Our aim was to explore the perceptions of Australian adults living with type 1 (T1D) and type 2 diabetes (T2D) about what is needed to end diabetes stigma and discrimination.
Methods
As part of a randomised, controlled online survey to evaluate Australian diabetes campaign videos designed to raise awareness of diabetes stigma, adults with T1D and T2D (N=875; 31% exposed to the intervention) were invited to provide free-text responses to an open-ended question: ‘What do you think is needed to bring an end to diabetes stigma and discrimination?’ Preliminary thematic analysis was applied to the qualitative responses (N=390; 45%).
Results
Qualitative respondents were: 56% women/female, aged 57+14 (Mean+SD) years, 58% living with T2D. More than half (59%) agreed that people with diabetes experience stigma/discrimination due to their condition. Suggestions for ending diabetes stigma focused on: 1) ceasing stigmatising messaging and behaviours: e.g., healthcare and government portrayals of people with diabetes as a ‘cost to society’; stereotypes linking diabetes, weight and “lifestyle”, and; using the term diabetes without differentiating between types, leading to public misconceptions; 2) interventions to address stigma: including community-wide awareness-raising (public, schools, workplaces) to dismantle misconceptions; positive portrayals of diabetes in the media; upskilling healthcare professionals; adoption of stigma-reduction policies (e.g., workplaces, airports, schools); increased safe spaces and community understanding of anti-discrimination rights. While some respondents minimised diabetes stigma as a concern, others believed that diabetes stigma will never be eliminated.
Conclusions
These findings suggest multi-level opportunities for collective and cross-sector action in the pursuit to end diabetes stigma and discrimination. Evaluative research on stigma-reduction interventions is needed urgently.
Meaningful inclusion of people with lived experience
These findings suggest multi-level opportunities for collective and cross-sector action in the pursuit to end diabetes stigma and discrimination. Evaluative research on stigma-reduction interventions is needed urgently.
Kweinorkie Tetteh- Quaynor, Diabetes Youth Care Ghana
An august visitor paid a surprise visit and after several bouts of infections over a period of two years, a diagnosis of type 1 diabetes was made. An unexpected new chapter that had to be embraced as there was no turning back. Insulin shots, regular hospital reviews, diet modification, exercising and literally living intentionally. This was a lot for a 10-year-old to soak in at the time, but I did my best.
Every single step of this journey has brought different experiences my way. From comments like:
I constantly had to explain with an attempt to clear these misconceptions from the clouded lens of these masses.
On the brighter side, diabetes opened me up to a world of healthy living, health consciousness, meeting other great individuals living with diabetes, sharing my journey and learning from others living with diabetes including my mother who has been living with diabetes for 27 years and has been an inspiration on this journey.
I lived through these experiences, completed medical school, also a proud a member of Diabetes Youth Care Ghana founded by Dr Nana Ama Barnes -Amoa, with other great volunteering physicians, and have since joined in mentoring other children living with diabetes, creating awareness and ironing out misconceptions that bring about stigma.
I hope to use my position as a medical doctor to increase access to diabetes supplies and to improve the lives of young people living with diabetes in Ghana irrespective of their location.
Author: Dr. Kweinorkie Tetteh- Quaynor, living with type 1 DM for 17 years, conquering this journey one day at a time. # diabetes won’t stop me.
Pedro Al Derjany, Dialeb
Since 2016, living with type 1 diabetes in Lebanon shaped my understanding of how deeply stigma can influence my daily life. Misconceptions often appeared in subtle ways… in school, in social situations, and even in healthcare settings. Before people understood my personality or abilities, they formed assumptions about what I could or could not do. These experiences affected how I viewed myself and led me to stay quiet about my condition for years.
Over time, I realised that silence allows stigma to grow. I began sharing my story with classmates, teachers, and community members. What started as simple explanations became an ongoing commitment to raising awareness and challenging inaccurate beliefs about diabetes. Speaking openly helped me understand the power of storytelling and how lived experience can spark change. Today, I continue this work as a Young Leader in Diabetes with the International Diabetes Federation representing my beloved country Lebanon and Dialeb and as an advocate with DiaLeb in Lebanon. I deliver awareness sessions, engage with medical students, participate in community activities, and contribute to discussions where the voices of people living with diabetes are often missing. These experiences reinforced my belief that stigma is not only interpersonal it is also systemic, shaped by social norms, access to care, education, and policy (we gradually miss them all in Lebanon).
My academic background in diplomacy and strategic negotiations strengthened this perspective, helping me see how systems, narratives, and institutions influence the experiences of people living with diabetes through advocacy so that advocacy will become a policy one say. I aim to integrate lived experience with a systems-thinking approach to support long-term change.
I hope to contribute to the Global Summit to End Diabetes Stigma in Jaipur by sharing my story, learning from others, and collaborating on solutions led by people with lived experience.

Richel Arthur, Diabetes Youth Care
I was born in Ghana, West Africa, some 22 years ago when there was little knowledge of type 1 Diabetes in children. I attended diabetes clinic with adults in their sixties when I was just twelve, the stares, the pity… the hospital felt like a second home. I didn’t understand what was happening, and my family didn’t either; to some, it was spiritual, to others, a matter of local herbs, or a test of faith.
There was always the “why me?” My mother would sob after checking my blood sugar levels, dress my wounds, and send me to school. There, I ate separately, tasteless meals prepared and served apart from other students. I grew up feeling different, even disliked, and often wondered if anyone truly understood me.
The cost of insulin was high. Some days I felt I was wasting money just to survive and during the pandemic, people bought insulin in bulk, causing a shortage. The fear of running out and the feeling of being a burden was my normal childhood.
Seeking freedom in adolescence, I read widely about diabetes and discovered Diabetes Youth Care (DYC), a local support group in my country where my advocacy began, determined to give young diabetics what I never had; a voice, care, and understanding. Even when neighbours accused me of doing illegal drugs for injecting insulin, I didn’t stop, holding on to my purpose.
My struggles fuelled my advocacy. I regularly grant television interviews on diabetes, go to schools to educate students on diabetes and then educate my fellow young diabetics during my local support group’s monthly meetings. Currently, I’m known as the “mother” in my local support group, drawing young diabetics close and checking on their caregivers to ensure they are supported. My hope came from the “blue hopeful circle” I found in DYC. The place that gave me courage, confidence, and the platform to stand up and fight the stigma I grew up with, so that no child feels alone or unheard.
Brittainy Hancock, Diabetes Action Canada
| Co-authors: | Fizza Abbas |
Background / Aim(s)
Language plays a central role in how people experience diabetes care. Many people describe clinical encounters where they felt judged, blamed or misunderstood, which can create shame, reduce trust and make it harder to be open about their experiences. This project aims to help nursing students and healthcare teams recognize how everyday communication can unintentionally reinforce stigma and to encourage more compassionate, person-centred care.
Methods
The initiative uses short written stories, voice notes and real-world examples from people living with diabetes to illustrate how stigma is reinforced in clinical settings. Personal experiences were gathered through a co-mobilization session with 25 participants who shared diverse lived and loved experiences of diabetes, and an ongoing survey continues to gather individual submissions. Early versions of the materials were presented at the 2025 Diabetes Canada Conference and will be further refined with input from a cohort of university nursing students.
To translate this knowledge into action, the project is developing a three-part nursing education toolkit:
Outcomes (achieved or expected)
Preliminary conversations with nursing educators suggest strong interest in the toolkit. Formal evaluation will begin once the full set of materials is piloted, with expected outcomes including deeper reflection on diabetes-related stigma, stronger communication skills in clinical encounters and greater confidence in using supportive, non-stigmatizing language.
Lessons learned (for scaling / adaptation)
We expect that simple, relatable storytelling will help learners connect emotionally without feeling blamed or defensive. Early interest from educators suggests that the toolkit’s modular structure is easy to integrate into existing curricula and professional development programs. The facilitation guide is designed to support adaptation across diverse healthcare disciplines and teaching settings.
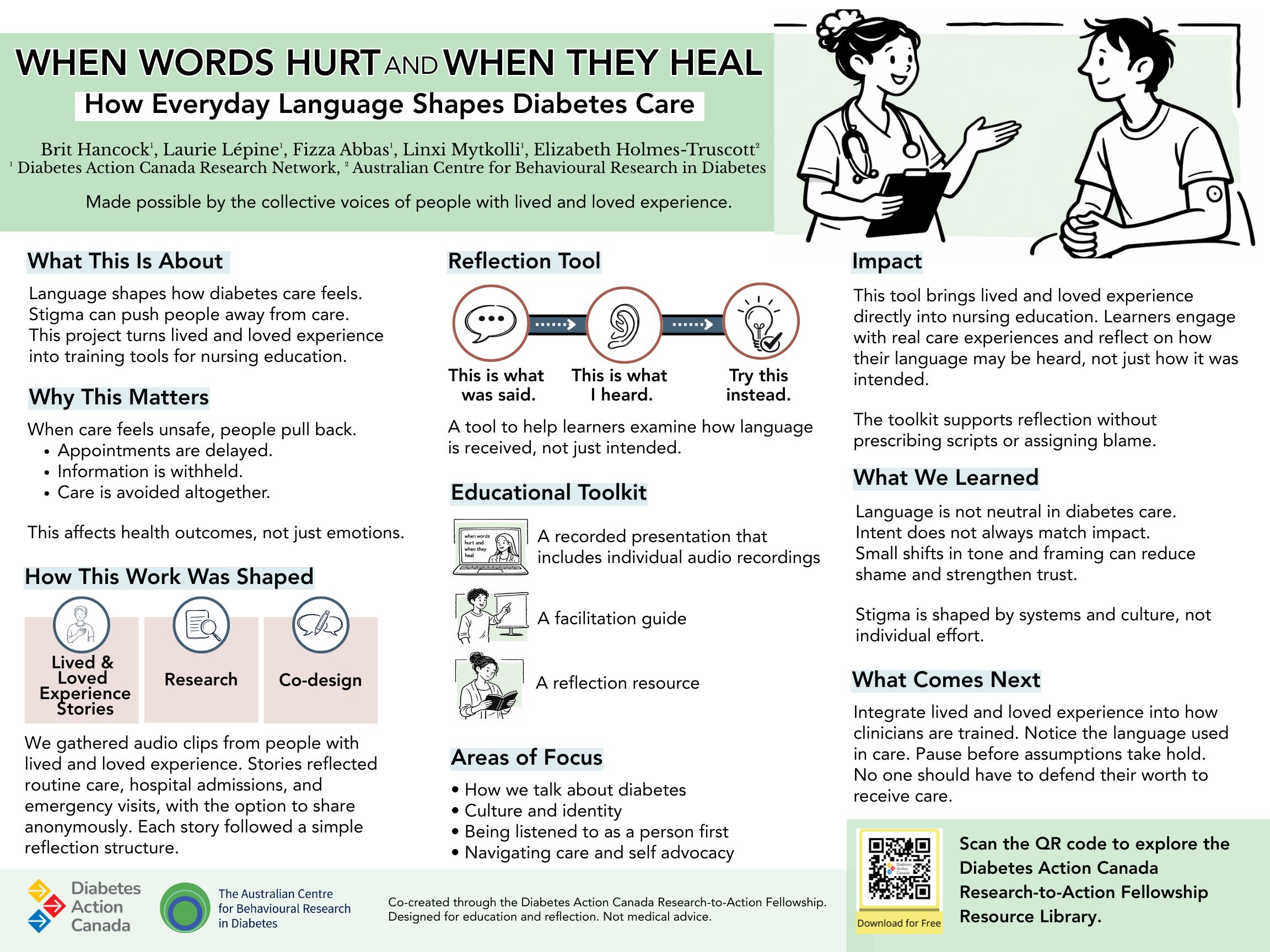
Susan Abraham, ECCQ
As a first generation migrant woman who has lived in Africa and Australia, I will use my lived experience with type 2 diabetes to highlight the importance of targeting migrants from high risk populations (eg South East Asian backgrounds). I will use my experiences from living with gestational diabetes and later progression into type 2 diabetes as a resident of 2 states in Australia to highlight how lack of culturally sensitive care can accelerate the progression of diabetes in high risk women. I will also share my story of how as a previous IT Engineer who made a career change into Public Health to raise awareness of the importance of improving one’s own health literacy and how workplaces such as IT companies can support people living with diabetes and help tackle diabetes stigma.
Mridula Bhargava, Diabetes Fighters’ Trust
I’ve lived with Type 1 Diabetes for 33 years. And let me be clear: the hardest part has never been the injections, the numbers, or the science.
It’s the assumptions.
When I got married and wanted a baby, nobody told me “you can’t.” But I could feel the quiet expectation — the cautious tone, the professional hesitation, the suggestions whispered to my mother instead of spoken to me.
“Maybe IVF.”
“Maybe diabetes is slowing things.”
“Maybe… maybe… maybe.”
Everyone had advice. I had a vision.
And I wasn’t alone. My husband and family stood beside me — steady, patient, unshakeable. Not once did they treat me like a fragile body. They treated me like the woman I am — strong, capable, and absolutely in charge.
Yes, the journey was long. Nine years long.
Three IUIs that failed.
One miscarriage that broke my heart but not my spirit.
Panic attacks. Hospital corridors. Tears no one saw.
But here’s the part that matters:
I didn’t stop.
I listened to my body, not the noise.
I trusted myself, not the doubt.
And in my own time — not society’s timeline — I conceived naturally.
Today, I have a beautiful baby and a family that fought with me, not against me. Diabetes didn’t block my life — it taught me discipline, focus, and resilience sharper than steel.
I’m sharing this because too many people still see diabetes as a limitation, a warning sign, a barrier.
I am living proof it is none of those things.
I didn’t “beat” diabetes.
I grew with it.
And I built a life I’m proud of — not despite it, but with it.
That is the story the world needs to hear.
Serena Akiki, International Diabetes Federation
Young Leader in Diabetes – International Diabetes Federation (IDF)
Communications & Advocacy Contributor – Chronic Care Center, Lebanon
Founder – teeoneedee (Digital Diabetes Awareness Platform)
I was diagnosed with Type 1 diabetes as a child, at an age when I barely understood the meaning of long-term health. What I did understand was the feeling of being different. At school, checking my glucose levels, carrying supplies, or stepping out of class often drew questions I wasn’t ready to answer. I learned early how isolating it could feel to manage a condition that few around me understood.
As I grew older, I navigated not only the physical aspects of managing diabetes but also the emotional ones: the pressure to appear in control, the fear of being judged, and the instinct to hide my challenges. It took years to realize that many young people living with diabetes shared these silent struggles.
Everything shifted when I began sharing my experiences on social media. What started as simple honesty became a space where others felt seen, heard, and supported. Connection replaced isolation. Storytelling replaced silence. Advocacy replaced fear.
Unexpectedly, opportunities began to unfold. I became one of the first young adults in the MENA region to appear in major diabetes awareness campaigns. I was invited to speak on television about my experience and the importance of understanding diabetes without stigma. Today, I represent both my country and my organization within the IDF, continuing the mission to amplify youth voices.
Social media remains my primary creative medium, where my lived experience and communication skills meet. Through my page ‘teeoneedee’, I use digital storytelling, visual content, and community-driven discussions to raise awareness grounded in empathy, and education.
My story is not about overcoming diabetes, but about embracing it as part of who I am, and using my voice to make others feel understood. By transforming personal challenges into digital advocacy, I hope to reshape conversations around diabetes with compassion, visibility, and dignity.
Alison Robinson, The Australian Centre for Behavioural Research in Diabetes
2021: a year of COVID restrictions, and for me, ten years with T1D and my third pregnancy. The pregnancy wasn’t easy, and I moved to a new town two weeks before giving birth. When I met my new obstetrician, they talked to a colleague about my baby having “large birthweight due to mother’s uncontrolled diabetes”. What that obstetrician didn’t see was the effort and sacrifices that came with having a pregnancy with diabetes. They didn’t see my glucose levels or HbA1c. They saw ‘diabetes’. They saw ‘large for gestational age’ (LGA). They assumed those two things meant uncontrolled diabetes – that I wasn’t trying, or that I didn’t care.
What that doctor also didn’t see was me crying afterwards from the sadness and frustration of not being seen. I felt guilt for bringing a baby into this world that was already affected by my diabetes. I was anxious about the care my baby and I would receive under this doctor, because I had kept my glucose levels in the target range, and yet this doctor didn’t see that. What else might they have missed?
I didn’t recognise these words as stigma at the time. And that was even after living with diabetes for 10 years, with a degree in health science and experience in research. It took me years to see that assumptions like this doctor’s, are stigmatising. Seeing the word ‘diabetes’ on clinical notes should not make people assume that means poor health or lack of effort.
I want to acknowledge the resilience it takes to live with diabetes – all types of diabetes – and to experience stigma, and still to persevere. People with diabetes deserve to be seen for who they are, and not for the condition they live with.
Description of the creative medium you are using: Short spoken story
Description of how people with lived experience of diabetes are/have been meaningfully involved: This is my own reflection of events that have happened to me as someone living with type 1 diabetes.
MANJUSHA BARVE, UDAAN
I was born into a home where illness was a constant companion. My sister had Type 1 Diabetes before she spoke her first words. My brother lived with cerebral palsy. Neighbours whispered that our family was cursed. I learned stigma not from textbooks, but from the way people looked at us — with pity, fear, and distance.
When I was fourteen, I began shrinking in front of my own eyes — thirsty, weak, losing weight. I checked my sugar on my sister’s glucometer. Diabetes.
And overnight, society rewrote my future.
“She won’t be able to study.”
“Her life is finished.”
“Who will ever marry her?”
These words etched themselves deeper than any needle.
But I fought. I learned to manage my diabetes and tried to keep my dreams alive. Then came the blow that nearly broke me — my brother’s death. I spiralled into depression and felt I had no strength left.
What saved me was finding a support group of young people living with T1D — a space where I wasn’t a burden, a problem, or a girl to be pitied. I was simply myself. They helped me rise from the inside out.
I sought therapy.
I studied harder.
I earned my degree in nutrition.
I lived independently in a hostel.
I rebuilt myself piece by piece.
When I felt strong again, I returned to the same community — but this time as a nutritionist, counselor, and advocate. A girl once written off now guides others through the same darkness she survived.
Stigma tried to define me.
Instead, it defined my purpose.
I rose — and now I help others rise too.
Calum Skye, Lived Experience Advocate
I was diagnosed with Type 1 Diabetes aged fourteen, I had never heard of diabetes, never known anyone with it and had no idea how it would alter my life completely.
Overnight, everything changed.
I had to learn how to treat myself, how to use all the equipment I was given and I often wished that my diagnosis was a mistake and that life could be ‘normal’ again.
But the stigma hit harder.
My planned future in the Royal Navy disappeared instantly, I was no longer deemed ‘good enough’.
Food, once enjoyed, became something I feared. Diabetes even managed to shape my diet!
I wasn’t just ‘Calum’ anymore; I was ‘Calum with Diabetes.’
My mood swings were misunderstood; accusations of attention seeking and being told there was nothing wrong with me.
Overtime my friends turned their backs on me until I felt alone, trapped within an illness that I couldn’t escape.
Everything became numbers and routines, as I attempted to hold myself together.
I lost myself, my identity and my future.
I was falling apart.
It was at this point in time that my mental health really took a hit, I was depressed and feeling suicidal, my dad recognised my struggles and began fighting to get me some mental health support, the support that should have been there from diagnosis!
What I’ve learned is this:
Stigma doesn’t just follow you; it shapes you.
Stigma convinced me that I was a problem.
Stigma made my diabetes feel like a monster I could never control.
However, with support, from professionals, family and friends, I began to reclaim myself.
Interaction with other individuals with diabetes has been the main catalyst for positive change.
Peer support and mental health support are a necessity.
NO ONE should have to face diabetes, or its stigma, ALONE.
Sayli Jadhav, Independent researcher
Sayli grew up in a world where diabetes was a common, almost inevitable part of life, an ailment woven into the family fabric. It was accepted, managed, but rarely discussed openly, reflecting a broader cultural reluctance to talk about illness. Interestingly, the women on her father’s side were the only ones spared the condition and were often seen as rude / not too well-behaved. This had nothing to do with diabetes of course but they weren’t the norm in the house.
For Sayli, this condition felt like an unavoidable inheritance, a certainty she knew she would receive. When the diagnosis finally came, her immediate fear was her parents’ reaction, and a deep yearning for simple reassurance: “It would be okay.”
The diagnosis drastically changed her life. Always being “different” or “weird,” diabetes was another thing added to the list, forcing her to live differently not only from her past self but also from her peers.
She describes diabetes as the child you wish you didn’t have: requiring constant care, prone to tantrums, and demanding a ceaseless balancing act. While she learned to live with it, the casual remarks of others often felt like a sharp prick—a painful realization that they saw her through the lens of her illness.
However, this is only part of her story. Over the years on this journey, Sayli has met many people and gained profound insights. She learned about her body, the world, and most importantly, how to truly care for and love herself. Her journey has recently led her into the challenging terrain of stigmaland. Equipped with a new lens, she now perceives social interactions that expose power imbalances related to her health. Uncovering deeper truths about human relationships as she continues to navigate the complexity of this life.
Jeffrey Bowser, dStigmatize/A Spoonful of Laughter
| Co-authors: | Shae Puckett; Matthew Garza |
https://www.youtube.com/watch?v=V8Yc76ksmVU
It was 2020, the height of the pandemic, when our nine-year-old daughter Eily was diagnosed with type 1 diabetes (T1D), and our lives were changed forever. However, I wouldn’t learn the extent of it until later. The books I devoured in the months that followed, and even Eily’s endocrinologist, failed to impart the devastating effect this disease would have on our little warrior’s mental health and the emotional strain it would take on our family. There were glucose monitor alarms disrupting class, a budding relationship with the school nurse, pump malfunctions, and dangerous lows in the middle of the night that threatened her safety, and our sanity.
And stigma.
A stranger’s offhand comment, the judgmental sideways glance from a flight attendant, and the arrogant ignorance of a swim meet referee. Every seemingly innocuous interaction further isolated Eily and reminded her she was different.
So, five years later, I wrote ‘The Bad 1’, short film as a love letter to Eily and T1s everywhere desperate to be seen as more than their condition. The silent movie genre seemed perfect to take a satirical swing at isolation, stigma, and antiquated attitudes surrounding T1D, and stress the importance of human connection to combat it. I’m partnering with the Spoonful of Laughter initiative to bring the message to the masses and hit the short film circuit. With official selections, one award, and a viewer who, “finally felt seen”, the response to ‘The Bad 1’ has overwhelmed me.
My obsession with helping T1D families continues to grow. This winter, I return to school to earn my Master’s Degree in family therapy. Weaving together my storytelling skills and future as a Professional Counselor, I’m going all in.
Shailesh Desai, Diabetes Canada
As a South East Asian person who has lived in Canada for more than thirty years, my health journey reflects both cultural expectations and the realities of chronic illness. For over twenty-five years, I have lived with Rheumatoid Arthritis, an early reminder that illness reshapes identity, mobility, and how others perceive you.
A decade later, diabetes entered my life—another autoimmune condition with its own stereotypes. At 6’2” and 80 kg, I did not fit the image many associate with diabetes. Comments like “You don’t look diabetic” or “What did you do wrong?” reduced a complex medical condition to personal blame. These misconceptions were not only inaccurate but emotionally isolating.
For more than ten years, I have also lived with depression and anxiety, experiences rarely acknowledged in diabetes conversations despite their strong influence on motivation, self-care, and the courage to seek support. In many South Asian and immigrant communities, mental health remains a taboo subject, making stigma even heavier.
In 2019/2020, a myocardial infarction followed by bypass surgery made diabetes management a central part of survival. Recovery brought vulnerability but also clarity: stigma thrives in silence, and silence limits understanding.
I share my story to promote open dialogue, humanize chronic illness, and challenge assumptions that harm more than they help. Diabetes, autoimmunity, heart disease, and mental health are not failures—they are complex medical realities that deserve empathy and informed conversation.
As a pharmacist and research collaborator, I have seen how lived experience can shift attitudes, support better care, and inspire meaningful action. Through honest storytelling, my goal is to create connection and ensure that others feel seen, understood, and less alone.
Daniela Rojas, Vaso LLeno
| Co-authors: | Cristina Gomar |
Most medical publications and scientific research on diabetes primarily emphasize clinical data and health outcomes. While this knowledge is essential, it can unintentionally underrepresent the lived experiences of people living with diabetes (PLWD) the everyday realities that influence emotional well-being, relationships, identity, and social inclusion. As the saying goes, “what is not named does not exist.” When emotions, concerns, and challenges are not acknowledged, they may remain unseen and insufficiently addressed within care systems and broader society.
Vasoterapia Diabetes is a participatory, card-based game designed to center lived experience in a respectful and supportive way. Its purpose is to create inclusive, psychologically safe spaces where participants can explore, share, and reflect on emotions and experiences related to living with diabetes. Through guided, voluntary conversations, the game encourages personal reflection, active listening, and recognition of shared experiences that are often difficult to express in traditional settings.
By fostering empathy, understanding, and respectful dialogue, the game supports meaningful communication among participants, including people living with diabetes, caregivers, and others in their support networks. It contributes to reducing diabetes-related stigma both societal and internalized by normalizing conversation and promoting understanding. Outcomes include increased emotional awareness, improved communication, and support for more holistic, person-centered approaches to care.
Each card includes carefully designed, evidence-informed questions that invite storytelling and shared reflection. The game format reduces barriers to participation, supports autonomy, and promotes emotional safety across clinical, community, academic, peer-to-peer, and organizational contexts.
Ciara Stevens, Nova Scotia Health
In March, I will have lived with type 1 diabetes for 28 years. I’ve seen and felt the effects of diabetes stigma both personally and professionally as a registered nurse. My passion for ending stigma comes not only from my own journey, but also from growing up with a father who lived with severe mental illness. He had schizophrenia, and I believe stigma played a role in his reluctance to seek care, and ultimately in his death. That experience taught me how deeply stigma can harm, and why eliminating it is essential.
At the End Diabetes Stigma Global Summit, I will use storytelling as my creative medium to share how I work to abolish stigma within healthcare and beyond. My stories will include experiences as a person with lived experience, and as a diabetes nurse educator. These stories will highlight my diabetes stigma experiences and responses.
I have spoken locally and nationally to healthcare professionals about diabetes myth-busting, stigma, and our role in eliminating it, not perpetuating it. This month I’ll be speaking about diabetes stigma at the Diabetes Canada Conference and next year at the Diabetes and Mental Health Conference. I recently received a Diabetes Canada Volunteer Award for my work as nurse coordinator at D-Camps, where I lead conversations about stigma, shame, and blame, and for serving as lead model in the Pump Couture Fashion Show, an initiative to change the conversation around diabetes.
For Diabetes Awareness Month, I developed a practical tool for healthcare providers to guide stigma-free care. In the future I’d love to be involved in research about diabetes stigma and in creating workshops to integrate diabetes stigma-awareness into healthcare training. My ultimate career goal is to see the end of diabetes stigma, and I will be putting in the work to make it happen.
Thapelo Semenya
Growing up with type 1 diabetes from the age of six shaped my entire world, but stigma taught me to make myself smaller. In school, I became “the girl with the needles,” watched by classmates, whispered about by teachers, and judged by people who assumed diabetes was caused by something I had done. As I shared in my diaTribe story, the hardest part was not the injections or the monitoring, it was the shame that others projected onto me. It made me believe my condition was something to hide.
Everything shifted when I found community. Hearing stories that mirrored my own reminded me that lived experience is powerful, not shameful. Storytelling became my way back to myself, a tool to reclaim confidence, connection, and visibility. It also became the foundation of my advocacy.
My ongoing involvement with the WHO Global Coordination Mechanism (GCM) on NCDs has strengthened this journey. Being in a global space where lived experience actively shapes discussions, priorities, and recommendations has shown me how meaningful inclusion should look everywhere. It has affirmed that people living with diabetes must be partners, not token participants. Our voices are essential to changing harmful narratives and dismantling stigma at every level.
This story brings to life the emotional and social impact of diabetes stigma while highlighting the resilience of the community. It challenges misconceptions by centring humanity, honesty, and the right to be fully seen. Through storytelling, I hope to inspire action, deepen empathy, and encourage systems to value lived experience as a driving force for change.
Lurina Fourie, The Glucose Glitch
This is the lyrics of a song I wrote, sharing feelings about diabetes stigma and discrimination and rising up, above it all. The actual song was created further with AI. Herewith a link to listen to the song on: https://youtu.be/16ACARgAwIg?si=o9r84y3FQ410HY23 – it was played at the IDF World Diabetes Congress in Bangkok earlier this year – when the IDF Young Leaders in Diabetes walked onto the stage to represent their countries.
The lyrics can also be used as a poem.
Harsh Pandya, Hoschule Anhalt: University of Applied Sciences
The thesis, Visualizing Wellness, utilizes quantitative health data and explores the possibility of representing its impact on qualitative aspects of life for a person with Type 1 Diabetes. It begins by examining the existing global stigma surrounding this condition and questions the efficacy of traditional health awareness methods.
The research delves into the relevance of data in our lives and its contextual importance in understanding the nuanced realities of living with invisible chronic conditions. The study then investigates existing data visualization practices from a creative lens.
The proposed design, Echoes of Control, is a screen-based audio-visual interaction inspired by graphs seen in continuous glucose monitoring systems. It replicates an important aspect of daily diabetes management; keeping sugars in-range.
Through sensorial engagement with a gamified version of the graph, it aims at informing about Type 1 Diabetes with the intent of starting meaningful dialogues, fostering empathy, and raising awareness.
By combining data visualization with storytelling, the intent is to open new avenues for thinking about diabetes, not only as a medical condition governed by numbers, but also as a lived experience.
This thesis explores how health data, when creatively represented, can become a medium for empathy, awareness, and dialogue.
The design proposal, Echoes of Control, is an audio-visual interactive and gamified graph, primarily aimed at informing non-caregivers about a daily aspect of Type 1 Diabetes.
Keywords: Type 1 Diabetes. Health Awareness. Empathy. Data Visualization. Storytelling. Interaction Design.d dialogue.
Stephen (Mark) Tiller, PSAD Study Group, Abbott Freestyle Libre Ambassador, Member of Diabetes UK Stigma panel, dedoc Voice
Failure is a human mental construct. It is not a physical thing, there is nothing you can point to and say “That is failure.”
You can only ‘fail,’ if you FEEL you failed. Have I felt that way in the past? Certainly I have, but I learned to look at it as learning the solution to a problem other than the one I was trying to solve. So, I didn’t ‘fail’, I just learnt that what I tried wasn’t the solution to my problem. I CHOSE to see it as an opportunity to learn something.
If someone stigmatises me or tries to tell me I am a failure, I can choose to accept that or I can choose to react differently, maybe just ignore what I KNOW isn’t true.
I can’t choose how other people act, but I can choose how I respond.
There is no failure, only feedback
Lurina Fourie, The Glucose Glitch
In this video, I use layers of clothing to represent the different layers of stigma associated with diabetes, to show how stigma can affect the people who experience it. It also highlights the positive impact of respectful language and how it can lead to better outcomes.
Sabrina Sosa Santa Ana, International Diabetes Federation
Creative medium
I am using a personal narrative essay to share a lived experience with diabetes, focusing on emotional insight and storytelling to convey its impact.
Meaningful involvement
The work is entirely grounded in my own lived experience with Type 1 Diabetes, reflecting authentic emotions, challenges, and perspectives.
Abstract
Diagnosed with Type 1 Diabetes at eight years old, I grew up in a childhood filled with love, friendship, and joy—far from the narrative of illness overshadowing youth. It was not until adolescence that the emotional weight of diabetes emerged. As my environment changed, I confronted social stigma, hurtful comments, and misconceptions. In retrospect, however, no judgment was harsher than the one I placed on myself.
During childhood, in-range glucose values earned me smiles and praise from my physician. As a teenager, the tone shifted. A single comment—likely forgotten by the doctor but deeply etched into my memory—became a turning point. His words, “Why should I tell you what to do if you’re going to do whatever you want anyway?” left me feeling voiceless, ashamed, and unworthy. I stopped attending medical appointments for nearly five years. That moment broke me, compounding the internal struggle and depression I had been trying to manage alone.
Through years of therapy, the support of loved ones, and empowerment from diabetes education, I rebuilt myself. I discovered my vocation and became my own hero. Today, I share my story to advocate for the mental health of people living with diabetes, to remind them that their worth is not defined by glucose numbers, and to fight the social stigma that delays acceptance and harms well-being. I encourage individuals to find strength within themselves and to use their voices—because words can wound, but they can also heal, educate, and transform.

Chris Lee, Mindirrima Cultural Solutions
The first documented case of diabetes in a First Nations person in Australia was recorded in 1924. Just over one hundred years later, First Nations Australians are experiencing some of the highest diabetes burdens recorded anywhere in the world. Our communities now lead the world in gestational diabetes, diabetes in pregnancy, and youth-onset type 2 diabetes— conditions that are emerging earlier in life and progressing more rapidly than in the wider population. Adult type 2 diabetes prevalence in some remote regions has been described as “among the highest reported of any population globally,” with rates approaching or exceeding one in three adults. Diabetes-related kidney failure, lower-limb amputations, and mortality rates also remain unacceptably high, with renal disease representing one of the most severe complications and amputation rates documented up to 38 times higher in certain settings. Diabetes mortality sits nearly five times higher than for non-Indigenous Australians, contributing significantly to the life expectancy gap.
Beyond its physical impacts, diabetes carries a profound social and emotional burden. Diabetes-related stigma—expressed through blame, shame, judgment, and harmful stereotypes—deeply affects how many First Nations people navigate their diagnosis, treatment, and identity. This stigma is reinforced across health systems, media representations, workplaces, and family environments. It leads to disengagement from care, reluctance to disclose diagnosis, psychological distress, diminished trust in mainstream services, and reduced capacity for self-management. These factors compound the already disproportionate rates of complications.
Ending the stigma around diabetes is essential to improving health equity. Effective responses must acknowledge the cultural, social, historical, and structural determinants shaping First Nations’ health. A shift toward culturally safe, strengths-based communication and community-led diabetes care is vital. Creating environments free from shame—where people feel respected, empowered, and culturally supported—is critical to improving outcomes and ensuring our people can live well with diabetes.
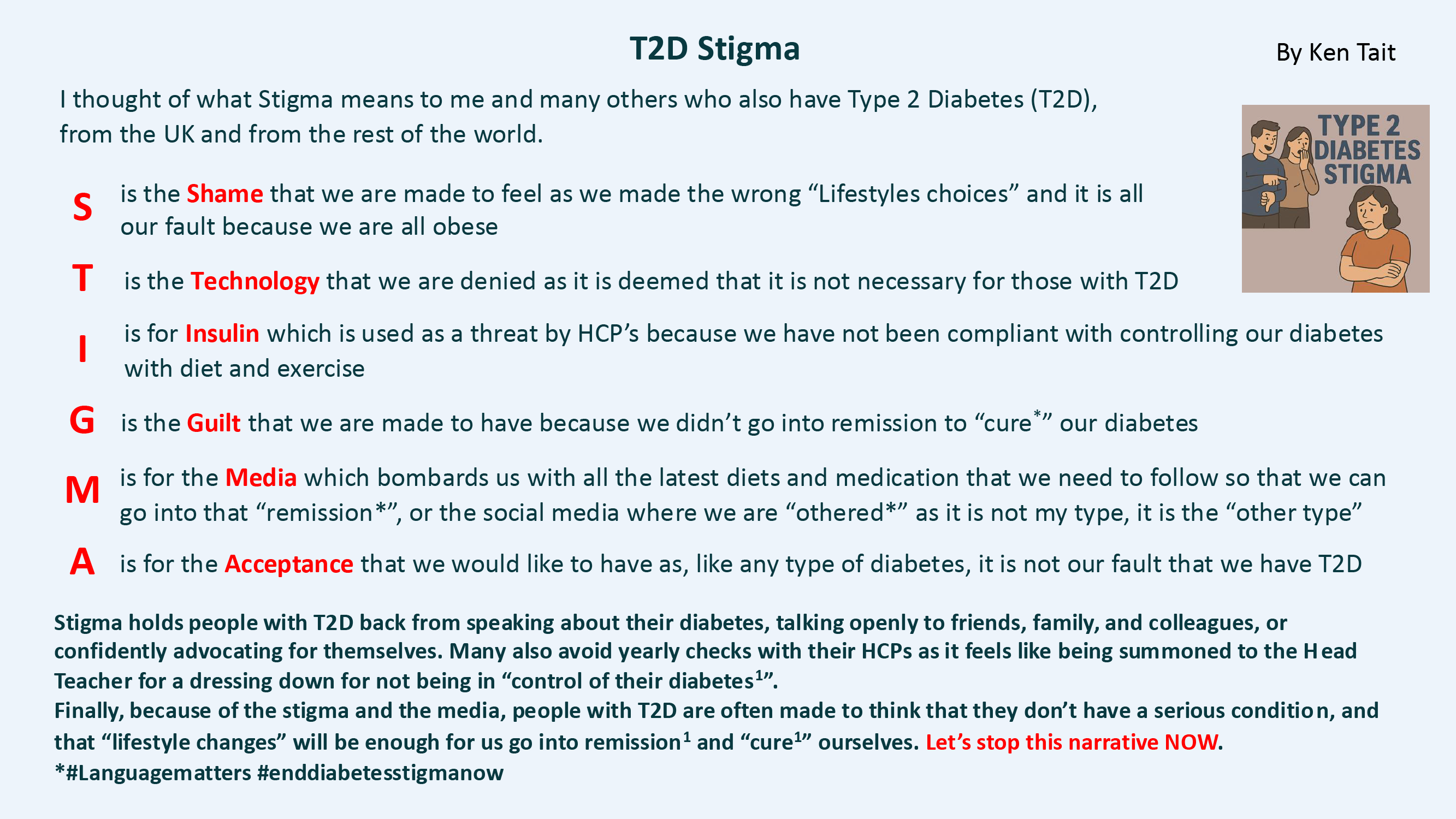
Kenneth Tait
Thinking about what stigma means to people living with type 2 diabetes and using the anagram STIGMA as a method of conveying this.
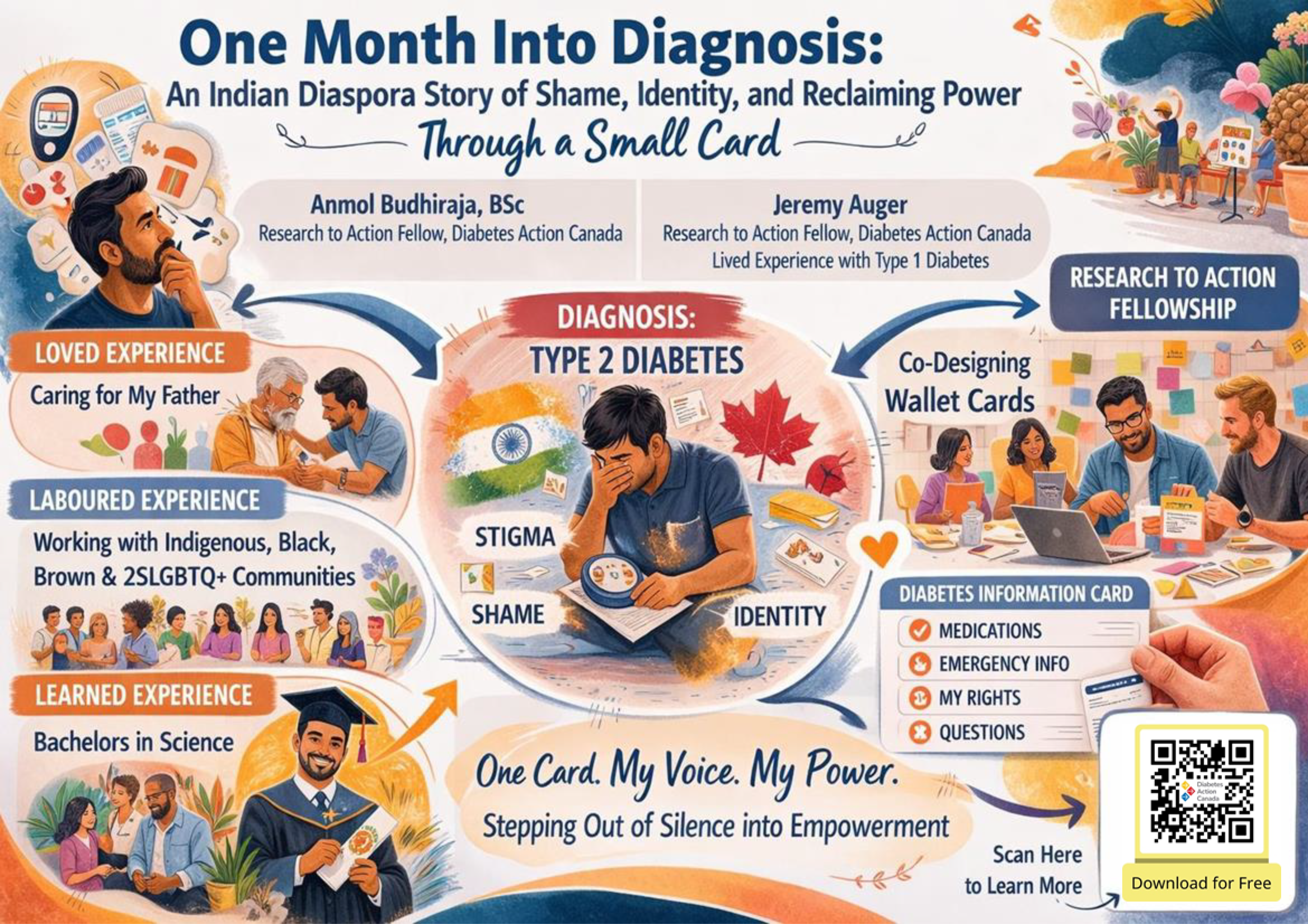
Anmol Budhiraja, Diabetes Action Canada (DAC)
We began creating our wallet-sized diabetes information card before I knew I would ever be diagnosed. I brought loved experience supporting family and friends, learned experience from my studies, and laboured experience from my work with people navigating chronic conditions. I cared deeply, but I was still slightly outside the circle.
One month ago, everything changed. My own diagnosis of type 2 diabetes carried more than medical meaning. As an Indian person who has lived in Canada for quite a long time, I feared telling my family back home. Past comments about my weight resurfaced, reminding me I should have taken better care, and the quiet shame that lingers in many Indian households made conversations feel impossible. Stigma made me afraid not of the condition, but of the dialogue it would force.
In Canada, I faced another layer of stigma shaped by racialized assumptions about my body and health. I found myself between two worlds, each marked by its own silence. Yet diabetes was not new to me: my family and loved ones live with it, and my work surrounds me with others navigating chronic conditions. Now, with my diagnosis, I carry lived experience alongside loved, learned, and laboured experience. The project became personal.
Together with my fellowship partner, Jeremy Auger, we designed a card small enough to hold secretly when shame feels heavy, but strong enough to empower someone during an appointment. The back lists your rights, giving voice to those unsure how to talk to their doctor.
This submission uses Indigenous art, reflective writing, and co-design input from people with lived and loved experience of diabetes stigma, particularly weight-based shame. Their voices guided every detail, ensuring the card informs and protects. This story is about one month, one diagnosis, and one card that helped me step out of silence. One day, I hope to bring this work back to India so others can feel the same courage.

Mark Odachi, University of Nigeria Nsukka
Have you ever heard a sentence passed long before you are even found guilty? This is my story with type 1 diabetes. I was diagnosed at 14, a year after my class teacher had warned that “if you have diabetes, you are finished.” Those words rang even louder when the doctor told my mom I was too young to have diabetes. The condition shaped my identity before I understood it. I was constantly pitied by family, friends, and others with goodwill, and this filled me with insecurities that affected how my family and I managed my diabetes because we all misunderstood it.
Four years later, I was withdrawn from the seminary because my superiors considered me too fragile. I was told, because of my diabetes, “You are not fit for this vocation.” It crushed me and the dream of becoming a Catholic priest, something I had wanted since childhood. I became a master at hiding my diabetes. I avoided talking about it, took my insulin in the toilet, and feared making excuses in class when I felt unwell or needed to use the bathroom.
But as my vocation to the priesthood closed, it became a turning point for me to learn more about diabetes. I soon realized it was not my fault. After sharing my story on a Facebook group, I met people with diabetes, and a journey I thought was mine alone became easier to navigate.
I later founded a support group called Diabetes Advocacy & Support Community (DASC) to educate, create awareness, and provide peer support for people with type 1 diabetes, ensuring no child or young person feels unworthy, alone, or unfit because of their condition.
Chris Toavs, University of Cambridge and T1International
After my diagnosis with type 1 diabetes, I threw myself into education and raising awareness in my local community. I was extremely outspoken throughout middle school and high school which earned me the nickname “diabetes girl”. In my pursuit of advocacy for safety and “normalcy”, I was labeled and cast as the punchline to crude diabetes jokes about consuming too much sugar. As one of the only people living with diabetes out of about 400 high school students, I wrestled with isolation and insecurity in ways I never anticipated. These feelings did not disappear after entering adulthood and encountering a plethora of misconceptions and prejudices beyond school buildings.
For the majority of my time living with diabetes, I didn’t know many people who were also living with this condition and battling the judgements of this world. To escape the stigma thrust upon me, I began writing poetry to capture my feelings of living with diabetes and perhaps connect with others like me some day. It has only been in the last year when I began working for a diabetes advocacy organization that I found a community who understands the delicate balance of managing blood glucose levels and navigating a complex cultural bias present both in and out of medical institutions.
The title of this collection of poems bears from my time using an insulin pump. Often my clothes/pants did not have pockets to hold my pump and was thus on display via a clip for the world to see. This reference, though, contains multiple facets drawing on my identity as a woman in a patriarchal world, a person living with diabetes in an ableist world, and a combination of the two as a woman living with diabetes in a biased healthcare system.
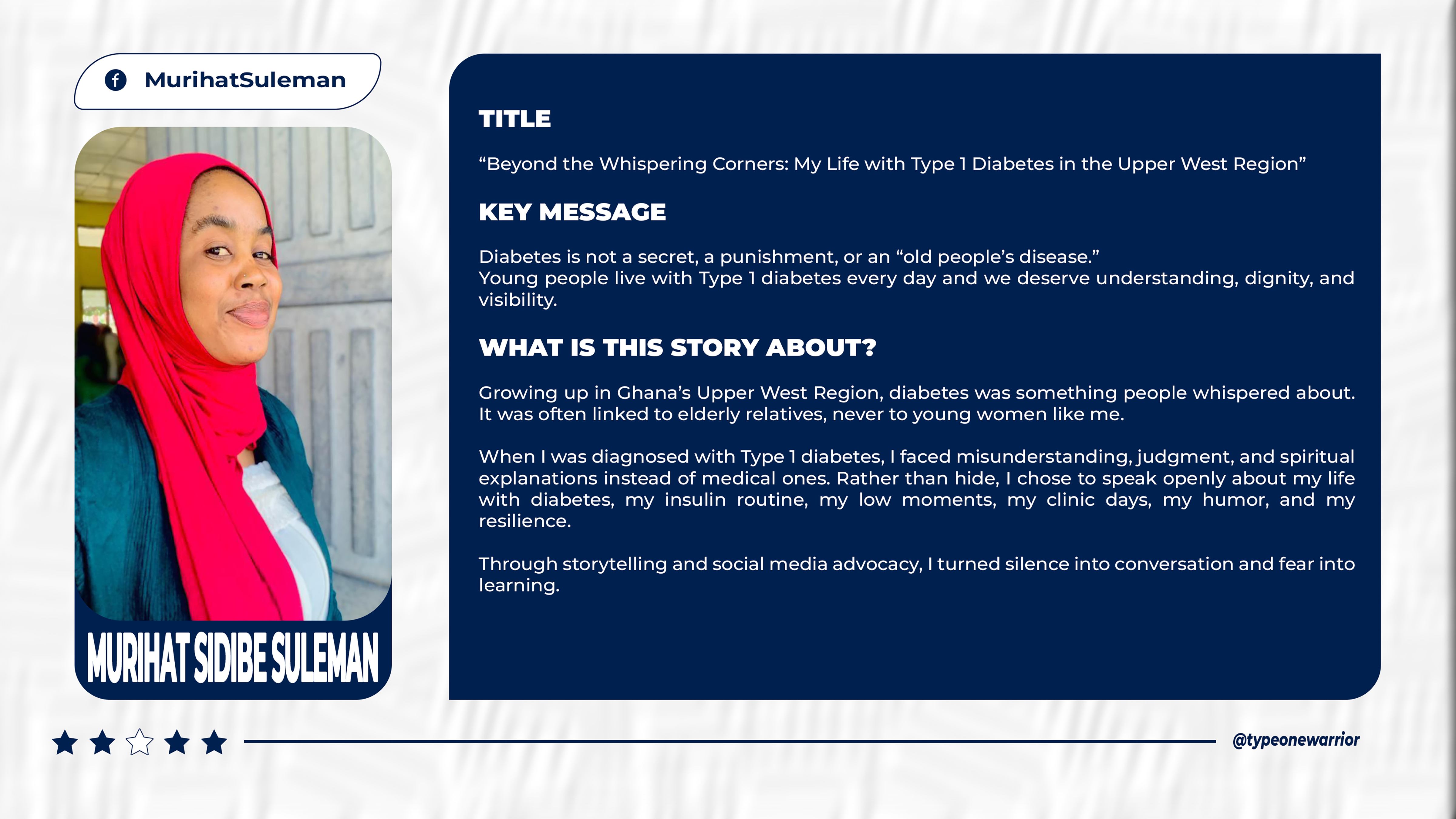
Murihat Suleman, Diabetes Youth Care Ghana
This presentation explores my lived reality as a young woman navigating Type 1 diabetes in the Upper West Region of Ghana, a place where conversations about diabetes often happen in quiet and misinformed corners. For many in my community, diabetes is seen as an illness of the elderly, not something that could affect a young woman. When I was diagnosed, I faced misconceptions, stigma, and spiritual explanations that overshadowed the medical truth. Instead of withdrawing, I chose visibility. I began openly sharing my daily routines my insulin injections, hypoglycemic episodes, clinic days, humorous moments, and the courage it takes to manage a chronic condition. Through social media advocacy, I created a relatable and educational space that challenged myths and invited genuine dialogue. Young diabetics began reaching out privately, grateful to see someone who represented their reality. Parents sought clarity, guidance, and reassurance. My storytelling demonstrated that Type 1 diabetes is not a death sentence and does not diminish a person’s dignity, capability, or dreams. By centering lived experience, this presentation highlights how personal narratives can shift community perceptions, encourage early diagnosis, and inspire empathy. Ultimately, my story is a call to amplify young diabetic voices and build a supportive environment where knowledge replaces stigma and every individual feels seen, understood, and empowered.
Harsh Pandya, Juvenile Diabetes Foundation
Storytelling has been the cornerstone of human culture. It is the primary vehicle through which we share experiences, transmit knowledge, and create connections. Today, storytelling transcends traditional boundaries, manifesting itself in movies, advertisements, product design, and digital media as a powerful medium to communicate complex messages with emotional resonance and clarity.
When addressing serious health conditions like diabetes, storytelling offers a transformative approach to dismantling stigma and misconceptions. It helps distill lived experiences into accessible, memorable verses that resonate across diverse audiences, illuminating the nuanced realities of living with chronic conditions.
Dia-Verse is a playful exploration of expressing diabetes experiences through the use of rhymes and poems. As the author and also a person living with Type 1 Diabetes, I bring authentic observations and experiences to these verses, addressing multiple dimensions of the diabetes journey. From navigating festivals and sports to cultivating self-awareness, understanding fundamentals, and adapting to new situations. Each poem serves as a window into the daily realities, triumphs, and challenges that often remain hidden behind clinical terminology and medical statistics.
This collection aims to bridge the gap between clinical understanding and human experience, offering youngsters with diabetes and their parents relatable narratives that validate their experiences while educating broader audiences. The scope of these poems extends beyond the written word, with potential for illustration, animated shorts, and published books that can reach diverse communities through multiple formats.
By harnessing the universal language of poetry, we can transform diabetes management from a solitary clinical obligation into a shared human experience, fostering empathy, reducing stigma, and empowering individuals.
Sweet Verses is a tribute to the Late Dr. Vijay Ajgaonkar, for being the guiding light at Juvenile Diabetes Foundation and beyond, and Late Alex Fernandez, for his love for writing about the achievements within the community.
Ebenezer Fletcher, Diabetes Youth Care
I was thrown into a brand-new world of diabetes management in November of 2014 at the age of 14 years. I was very confused and had no idea about what I was doing or how to do anything right. I recorded constant hyperglycemias and whenever I tried correcting them, I will end up with hypos. I developed boils and scars due to my inability to inject correctly. And my first HBA1C test recorded a 14.0%.
In February 2015, I was introduced to Diabetes Youth Care (DYC) which is a support network for young people living with Diabetes in Ghana. I started attending their monthly support meetings where I was taught to properly manage my condition and meet young ones like myself who motivated me to keep fighting for my dreams, I was assigned a mentor who checked up on me regularly and made sure I was adhering to my doctor’s instructions as well as managing my glucose levels the way I should. I was also provided with vital necessities for the management of DM like glucometers, test strips and insulin because they are difficult to get access to these supplies.
With the help of DYC, I have been able to learn so much from doctors, volunteers and diabetics alike which has drastically improved how I am able to take care of my self and warriors around me. I was able to record a 6.7% for my latest HBA1C test. I also don’t feel like being alone in this fight because DYC is always available to lend me the support I need. Through DYC’s push in advocacy, diabetes education in the country has also increased a lot which fights against stigmatization and empower warriors to not feel left out in their daily activities with the people around them.

Apoorv Jha
As a kid with T1D, I faced a lot of questions from my friends, relatives and closed ones. Some portrayed concern, some portrayed stigmas and misconceptions. Type-1 Diabetes or Diabetes Mellitus is not just an ordinary condition, it’s an auto-immune disease which changes lives for all the ones who are suffering with it. My story with Type-1 Diabetes began on 10th January, 2016. I was, like many, confused and unaware of what happened to me. There were days when I had breakdowns and tough times with my life. I faced bullying because of my condition, got stares for injecting insulin and mocked for carrying my glucometer while getting blamed for having a lot of sugars which led me to this. All of this because of lack of awareness.
I never wanted this condition to define me what I am not, I wanted it to show the world that what I can be. My goal in life is to create an impact in this world for which I am remembered. Type-1 Diabetes brought me a step closer to it. In 2020, I started Diabetes Advocacy by creating reels on Instagram about Type-1 Diabetes. I joined multiple organizations and initiatives and worked with fellow advocates to create awareness about this condition. I also helped newly diagnosed T1D Kids and teens to learn about Type-1 Diabetes. My work also got me a chance to be a #dedoc° voice representing India at ATTD 2024 as a Global Voice and a Tedx Speaker at Tedx Thaltej Youth 2025. For the first time in my life, I embraced my condition and moved with instead of going against it. Acceptance became my weapon which helped me impact not only my life, but life of others with me as a medium. Diabetes Advocacy starts with creating awareness about Diabetes and acceptance of the fact that T1D’s exist and live normally and its not their fault that they have it. It requires community efforts and it needs to be ubiquitous with the help of Social Media Platforms, Print Media and Key Figures speaking on the same.
Through my story, I want to show the world that “Nothing Changes in One Day, But One Day Comes when Everything Changes” and want to empower others to embrace their condition and let their condition define who they can be instead of who they can’t be.
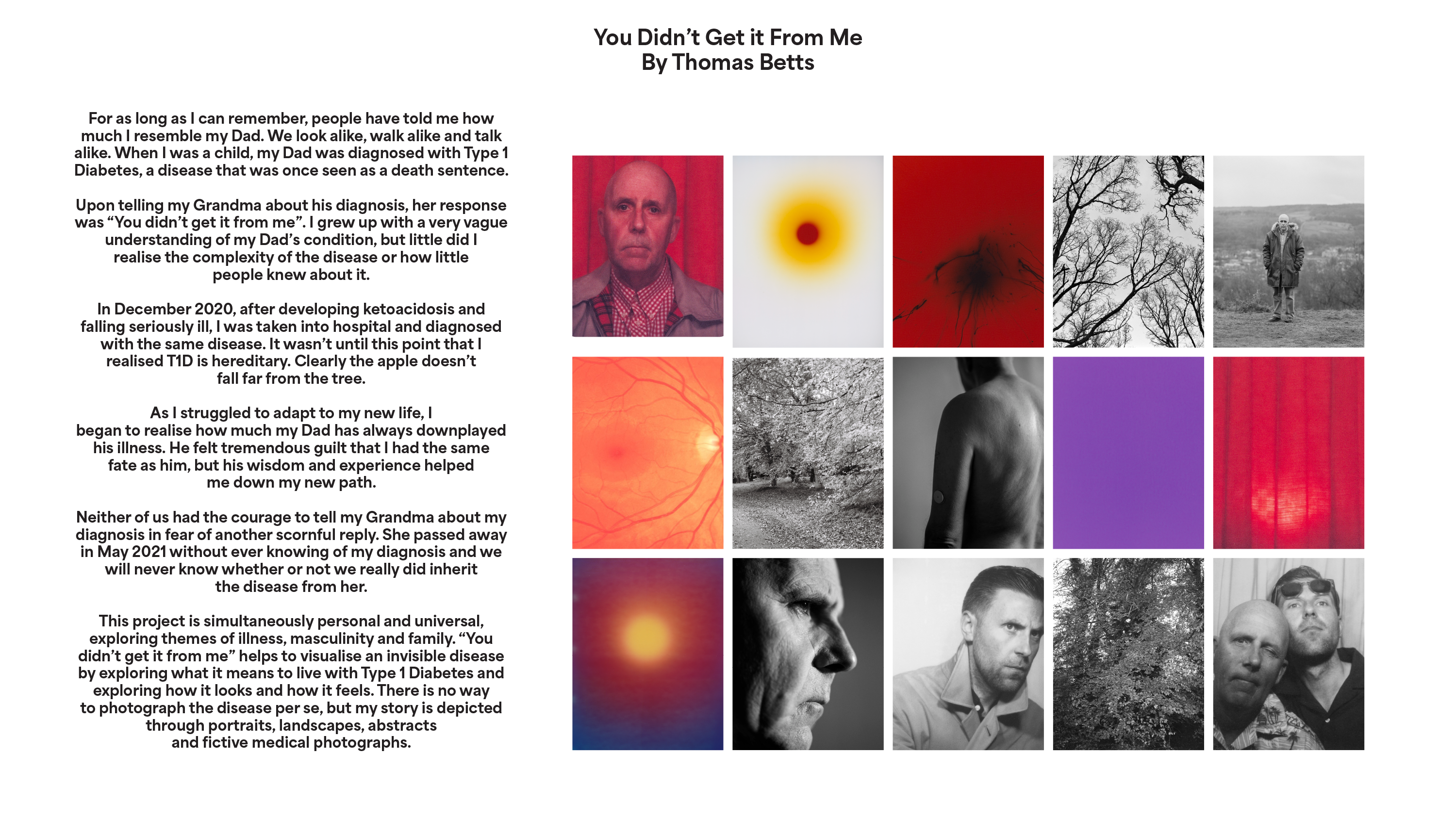
Thomas Betts
For as long as I can remember, people have told me how much I resemble my Dad. We look alike, walk alike and talk alike. When I was a child, my Dad was diagnosed with Type 1 Diabetes, a disease that was once seen as a death sentence. Upon telling my Grandma about his diagnosis, her response was “You didn’t get it from me”. I grew up with a very vague understanding of my Dad’s condition, but little did I realise the complexity of the disease or how little people knew about it.
In December 2020, after developing symptoms and falling seriously ill, I was taken into hospital and diagnosed with the same disease. It wasn’t until this point that I realised T1D is hereditary. Clearly the apple doesn’t fall far from the tree. As I struggled to adapt to my new life, I began to realise how much my Dad has always downplayed his illness. He felt tremendous guilt that I had the same fate as him, but his wisdom and experience helped me down my new path.
Neither of us had the courage to tell my Grandma about my diagnosis in fear of another scornful reply. She passed away in May 2021 without ever knowing of my diagnosis and we will never know whether or not we really did inherit the disease from her.
This project is simultaneously personal and universal, exploring themes of illness, masculinity and family. “You didn’t get it from me” helps to visualise an invisible disease by exploring what it means to live with Type 1 Diabetes and exploring how it looks and how it feels. There is no way to photograph the disease per se, but my story is depicted through portraits, landscapes, abstracts and fictive medical photographs.
Suman Bhagavathula, Voice Of T1D
When my child was diagnosed with Type 1 Diabetes (T1D), our family’s daily life quickly became centered on frequent finger pricks, insulin dosing, and continuous glucose monitoring – often requiring repeated interventions within a single hour during hypoglycemic episodes. Families across India and around the world live similar realities. Alongside these medical demands, many families face persistent diabetes-related stigma rooted in misinformation and harmful language.
We have personally encountered stigma in the form of statements suggesting that eating sweets causes diabetes, as well as ridicule implying that a child living with T1D is “suffering” and therefore limited in future aspirations – such as being told that pursuing a career in endocrinology would be unrealistic. These misconceptions are medically incorrect, profoundly harmful, and can undermine openness, self-confidence, and ambition in children and families living with T1D.
Rather than retreat in the face of stigma, my family and I chose to share our story openly. Motivated by lived experience, I aspired and personally invested in a project to advance a non-invasive glucose monitoring technology aimed at reducing pain, cost, and fear associated with frequent glucose checks. While the initiative highlighted the promise of patient-driven innovation, it hit disturbing roadblocks in the form of misrepresentations, and I faced challenges related to transparency, ethics, accountability and severe intimidation, illustrating how vulnerable families can be when navigating complex innovation ecosystems. I have refused to give up and continue pursuing my original ambition, which is even more important now when there is a need for a safe and reliable way to cross check Continuous Glucose Monitor data.
I call for compassionate justice, so that families and patient advocates can focus on advancing much-needed diabetes technologies rather than expending energy navigating systemic barriers or misinformation. By fostering ethical collaboration, transparency, and accountability, we can ensure patient-centered solutions reach those who need them most while simultaneously reducing stigma and empowering the T1D community.
In response to these challenges, together with my child, family, and community allies, I founded VoiceOfT1D, an initiative dedicated to confronting diabetes stigma, promoting accurate understanding of T1D, advocating for equitable access to technology, and supporting families across India, United States and the world.
Ebenezer Fletcher, Diabetes Youth Care
Being diagnosed with Diabetes Mellitus in November 2014 changed my life in ways I never expected. I was in my second year of Junior High School and had no prior knowledge about diabetes. My mother and I had to learn everything from scratch, how to manage my blood sugar, administer insulin and adjust to a completely new lifestyle. When I finally returned to school after being discharged from the hospital, my mother informed my teachers and classmates about my condition so they would know how to support me. Unfortunately, instead of support, I began to notice a shift in how people related to me. I was excluded from activities I once enjoyed, such as sports and cleanup exercises. Watching my friends play football while I sat on the sidelines made me feel singled out and different, but I tried to convince myself it would soon be over since we were close to completing Junior High.
In October 2015, after JHS, I gained admission into my second-choice Senior High School, a category B school in my region. I was excited because I would be attending with a cousin I was very close to and I looked forward to a fresh start. We bought everything I needed and I felt ready for a new chapter. However, just before I left for school, my mother informed the headteacher about my diabetes hoping that the school would be prepared. Instead, we were told that the school could not admit me due to my condition. Although the headteacher claimed the school was not equipped to care for me, we knew it was due to a lack of willingness to understand or accommodate diabetic students. Eventually, I enrolled in a category C school where I knew the school nurse, hoping for a more supportive environment.

Emmanuella Hormenoo, #dedoc°
It focuses on stigma and discrimination I faced, the challenges and stereotypes I believed when newly diagnosed due to ignorance and the subsequent impact. However, despite the hurdles the message alludes to the fight I undertook to expose the stigma and one I will continually fight.
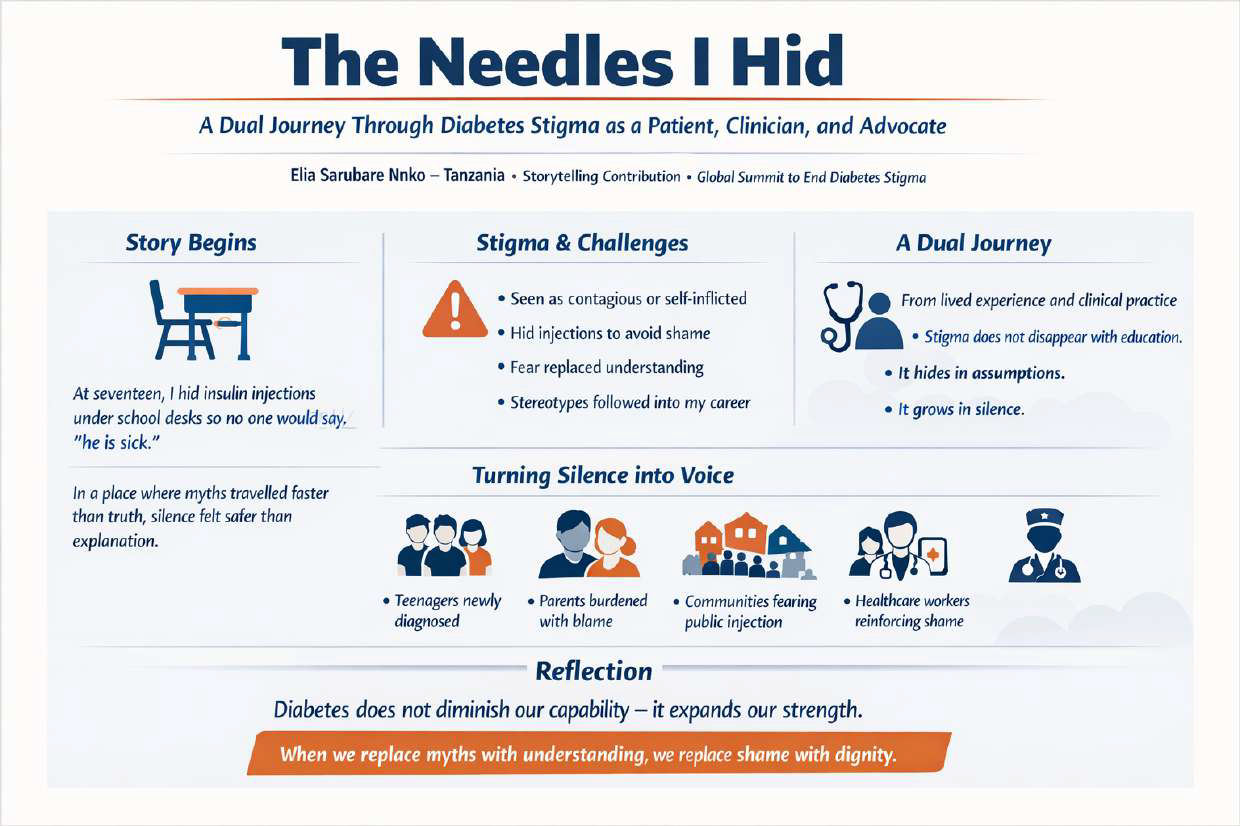
Elia Nnko, Independent Healthcare Professional & Diabetes Adv
At seventeen, I learned to hide my insulin needles under school desks so no one would say, “he is sick.”
I injected quietly behind classroom doors, carrying my diabetes like a secret I protected more than my own notebooks. People believed I brought this condition upon myself. Others thought it was contagious. Some simply stared. In a place where myths travelled faster than truth, silence felt safer than explanation.
Years later, I became a clinician — and the stigma followed me into the consultation room. Patients would look at the vial in my bag and ask, “How can a healthcare worker be injecting every day?”
Some colleagues whispered doubts about my abilities, as if Type 1 diabetes erased my training, my experience, or my worth. I realised then that stigma does not disappear with education. It hides in assumptions. It grows in silence.
But I also realised something else:
The very thing I spent years hiding could become the voice someone else desperately needed to hear.
So I began speaking.
To frightened teenagers newly diagnosed.
To parents who blamed themselves.
To communities where children still fear injecting in public.
To healthcare workers who unknowingly contribute to shame.
I shared my lived reality: eight years of managing Type 1 diabetes in underserved settings — storing insulin in improvised ways during power cuts, stretching limited supplies, navigating fear, misunderstanding, and the weight of daily survival. I told them that stigma hurts more deeply than the injections ever have.
Today, I speak not to highlight struggle, but to reclaim dignity.
To challenge the quiet harm of stereotypes.
To remind others that diabetes does not diminish our capability — it expands our strength.
Ending stigma begins with stories that refuse to stay hidden.
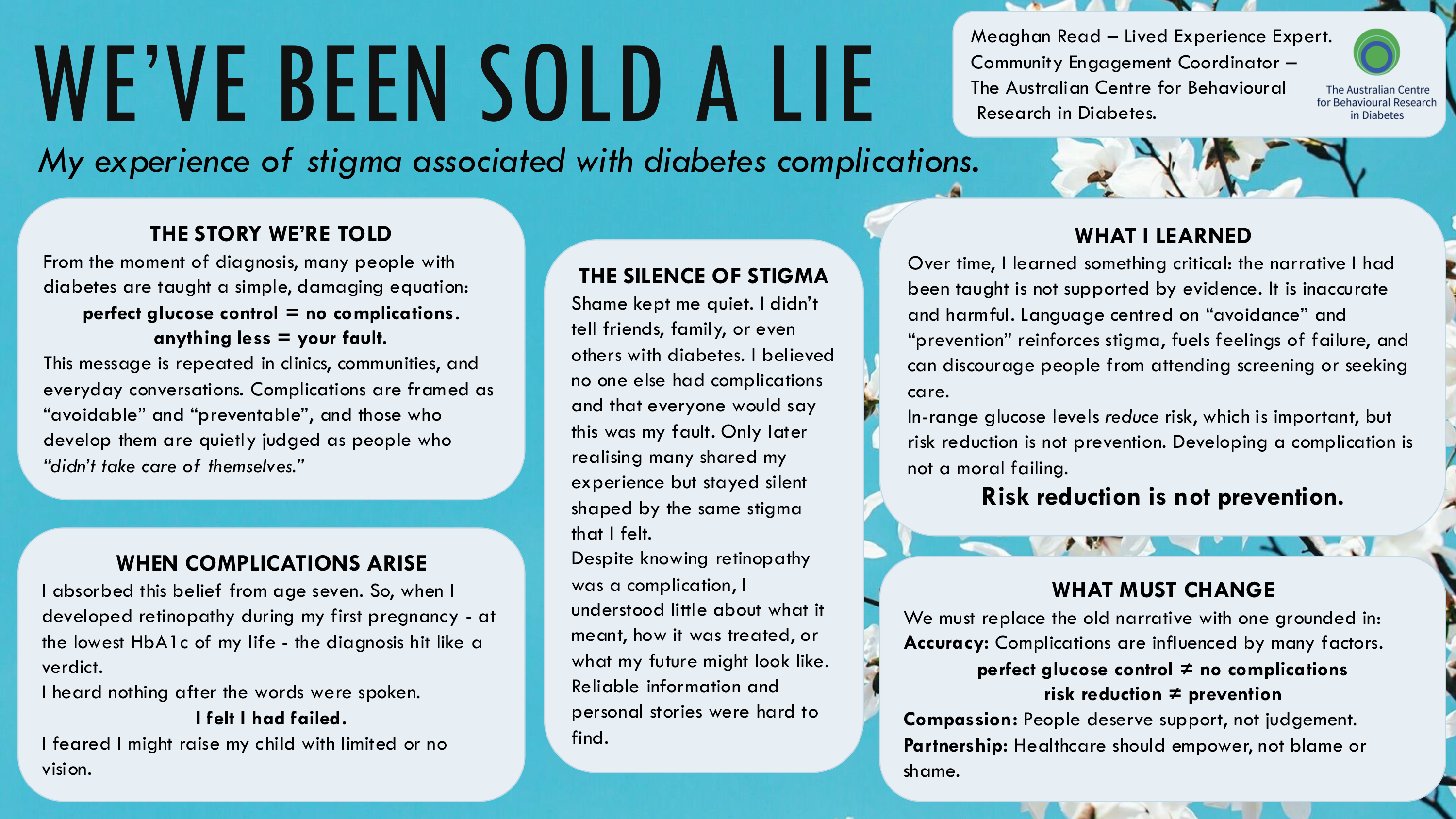
Meaghan Read, The Australian Centre for Behavioural Research in Diabetes
From the moment of diagnosis, many people with type 1 diabetes—including me—are taught a simple equation: excellent glucose control prevents complications; anything less leads to them. It’s a message repeated in clinics, communities, and everyday conversations. Complications are presented as avoidable through perfect effort, and those who develop them are often judged—quietly placed in the “didn’t take care of themselves” category.
I had internalised this narrative since the age of seven. So when, during my first pregnancy, at the point of achieving the lowest HbA1c of my life, I was diagnosed with retinopathy, the words hit me with devastating force. I heard nothing after the diagnosis. I felt I had failed—and that I might be raising my child with limited or no vision.
The emotional weight was compounded by isolation. I felt I couldn’t tell anyone without judgement, not even those closest to me. I believed no one I knew had experienced diabetes complications. Only later did I realise that others likely had—they just stayed silent, shaped by the same stigma I felt. And despite knowing retinopathy was a complication of diabetes, I understood surprisingly little about what it meant, how it was treated, or what my future might look like. Reliable information and personal accounts were hard to find.
Over time, I learned something critical: the narrative I had been taught is not supported by evidence. It is inaccurate and harmful. Language centred on “avoidance” and “prevention” reinforces stigma, fuels feelings of failure, and can discourage people from attending screening or seeking care.
In-range glucose levels reduce risk, which is important—but risk reduction is not prevention. Developing a complication is not a moral failing.
The narrative must be changed to one grounded in accuracy, compassion, and partnership rather than blame.
Nkiruka Okoro, NHS Greater Glasgow And Clyde
I was seven years old when my world split into two parts: before diabetes and after diabetes. Primary school should have been about multiplication tables, skipping ropes, and trading meat pies during break. Instead, it became a battlefield where my small body struggled to understand why it needed insulin to stay alive, and why my classmates whispered about me like I was a mystery wrapped in danger.
I still remember the day my teacher called me “the fragile one.” I was sitting at the front of the class, dizzy from a hypo, when she told the others not to “disturb the diabetic girl.” The label stuck. Children avoided playing with me for fear of “catching diabetes.” Some refused to sit beside me. Others stared when I brought out my insulin. At seven, I learned what stigma felt like—sharp, invisible, and capable of following you home. But I also learned something else: I carried a fire diabetes could not extinguish.
As a teenager in Nigeria, stigma grew heavier. People didn’t just misunderstand diabetes; they feared it. I was told, “Men don’t marry girls like you,” “You will be a burden,” “You cannot have children,” and “Who will care for you when you fall sick?” My worth, in their eyes, diminished because I needed insulin. I remember clearly when someone I cared for said his family rejected our relationship because I “might die young.” Not for lack of love or ambition—simply because I injected insulin.
Living with Type 1 diabetes became a barrier not only to health and relationships but to economic independence. Job applications demanding medical disclosure turned into silent rejection.
Somewhere between the whispered insults and the closed doors, I found purpose. Advocacy became my strength. Today, I stand not as the fragile girl, but as a survivor, professional, researcher, and resilient voice for millions.
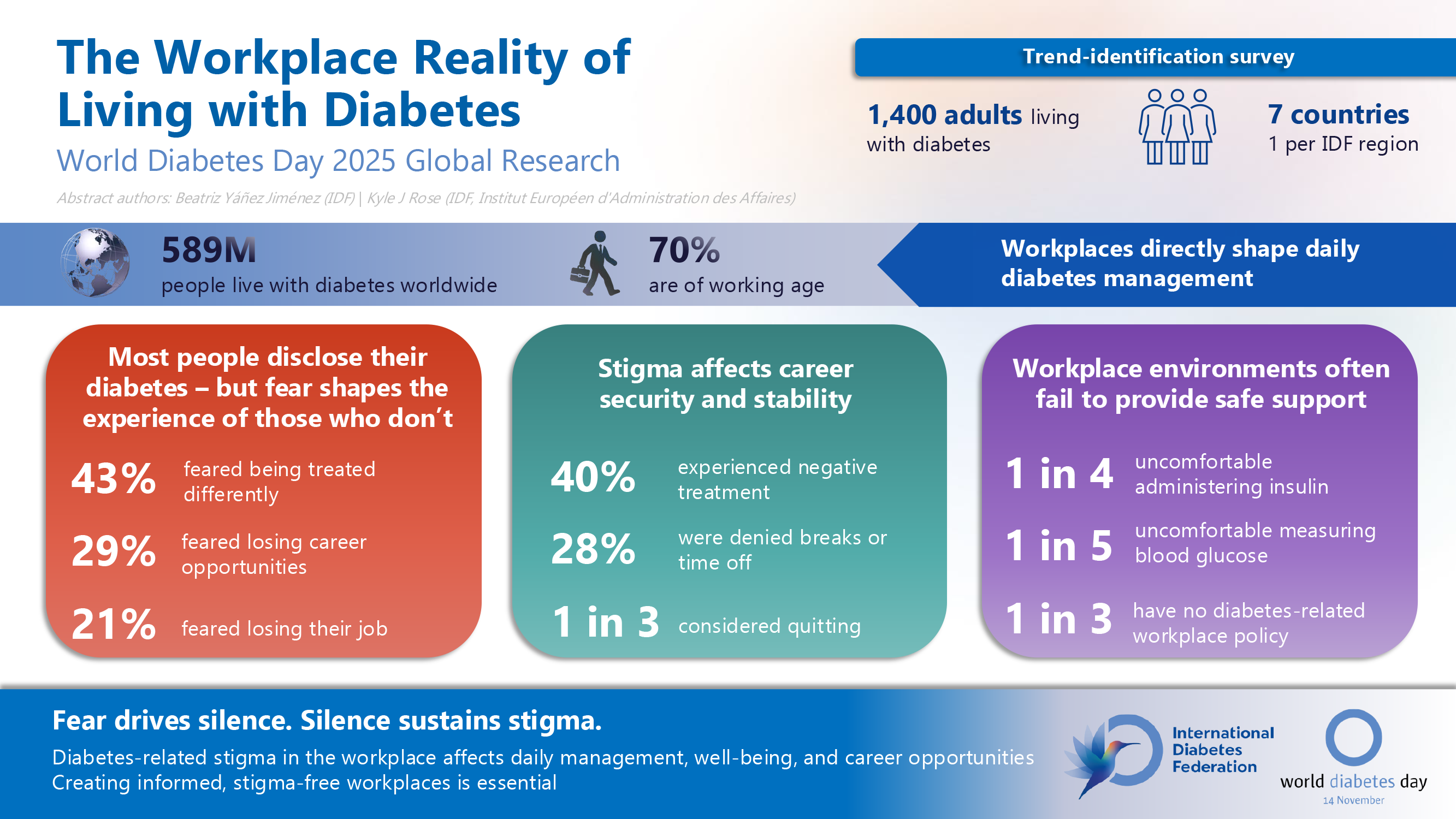
Beatriz Yáñez Jiménez, Diabetes Action Canada
| Co-authors: | Kyle J Rose |
Abstract
Around 70% of people living with diabetes are of working age. They face obstacles at work ranging from difficult access to medicine or food during the work day to discrimination about diabetes amongst colleagues.
In 2025, as part of ongoing research initiatives, the International Diabetes Federation commissioned Arlington Research, an independent agency, to survey 1,400 adults living with diabetes in seven countries around the world to better understand their experience in the workplace: Argentina, China, Germany, India, Pakistan, South Africa, and the United States of America. The people contacted were not representative of all people living with diabetes, nor for each of these countries; the respondents were contacted with the objective of identifying notable trends and patterns.
Our research indicated that many people living with diabetes do not feel comfortable addressing their own medical needs in their work environment. Many face stigma and discrimination on a daily basis.
Nearly half [46%] of employees diagnosed with type 1 diabetes reported negative treatment in the workplace, compared with just over a third [36%] of workers living with type 2 diabetes. More than a quarter [28%] reported having been denied breaks or time off to attend to their diabetes management. In addition to its emotional and professional impact, the findings show that diabetes-related stigma can also limit career opportunities. Almost a quarter [23%] said they had missed out on career development or training opportunities because of their condition. These barriers are compounded by a culture of silence. One in ten employees living with diabetes has not disclosed their condition to their employer, with 43% of those saying they feared being treated differently. Nearly a third [29%] of these respondents were concerned that disclosure could limit their career progression.
Many employees living with diabetes continue to rely on peer-level support. Close to one in three [29%] have confided in just one trusted colleague, while a slightly higher number [41%] have shared their diagnosis with just a few people at work.
The study also found that daily diabetes management is a source of anxiety for many employees. One in four respondents [26%] were not comfortable administering insulin at work, while one in five [20%] felt the same about checking blood glucose levels.
Conclusion
Our research reveals how deeply fear and stigma shape life at work. The vast majority of employers aren’t doing enough to provide stigma-free work environments for people living with diabetes. This hasn’t improved and the status quo is clearly impacting people’s quality of life, job opportunities, and safety in the workplace.
When asked why those who do not disclose their diabetes , people living with diabetes repeatedly used the word “fear”: fear of being treated differently, fear of being passed over for promotion, fear of harassment, and fear of losing their job.
The numbers above highlight the discomfort in addressing diabetes through formal workplace channels and underline the need for organisations to create more supportive and inclusive environments. Without adequate support, routine medical needs of individuals can become daily challenges in the workplace, imposing unnecessary stress on employees with diabetes.

Allison Nimlos, The Diabetes + Mental Health Conference
Background
The Diabetes + Mental Health (D+MH) Conference debuted in 2022 to address gaps in education about the effects of diabetes on mental health. The conference promotes mental health literacy, teaches evidence-based strategies, and provides a safe space to discuss issues often overlooked in traditional healthcare. D+MH educates attendees on how diabetes stigma negatively affects mental health and equips providers and people with diabetes (PWDs) with strategies to address stigma across settings.
Methods
The fully virtual conference includes keynote speakers, educational sessions, and interactive discussions. Dual tracks serve healthcare providers and PWDs, but attendees are encouraged to attend any session. The planning committee and faculty include PWDs, reflecting a “nothing about us without us” approach. Sessions address stigma and provide practical strategies for application across diverse settings. Faculty are encouraged to speak to all types of diabetes to foster inclusivity and connection and reduce stigma within our content delivery.
Alongside individual support, wmore and do more for diabetes at work’ and used creative methods to engage on the messages.
Outcomes (achieved or expected)
Lessons Learned
Healthcare providers and PWDs benefit from a collaborative, mental health conference. Providers are eager to understand stigma’s impact and strategies to address mental health. Faculty with lived experience enhance messaging and make content more meaningful for both PWDs and providers.
Lived Experience Involvement
PWDs serve as keynote speakers, session facilitators, panelists, and committee members. Their insights shape session design, guide discussions of stigma, and ensure messaging reflects real-world experiences.
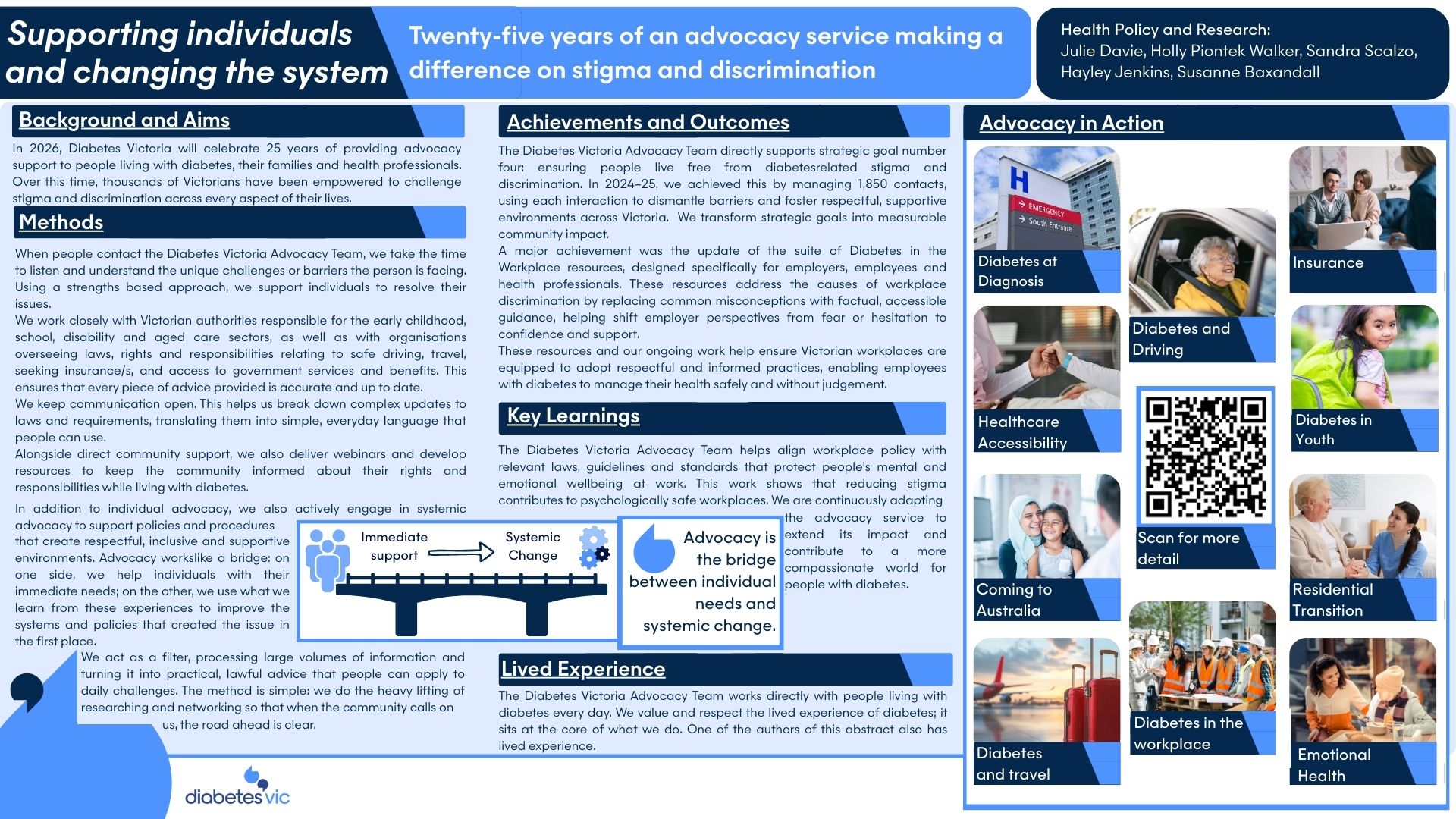
Holly Piontek Walker, Diabetes Victoria
| Co-authors: | Julie Davie; Susanne Baxandall; Hayley Jenkins; Sandra Scalzo |
Background / Aims
In 2026, Diabetes Victoria will celebrate 25 years of providing an advocacy service to stand beside people living with diabetes and their families. The service has provided support to thousands of Victorians by stepping in to help challenge stigma and discrimination in all areas of public life.
Methods
Our advocacy service helps with problem solving on a concern presented by an individual with diabetes, their family or their health professional. We take the time to listen to each person’s story, help them identify the unique challenges or barriers they are experiencing and use a strengths-based approach support them to resolve the issues.
Alongside individual support, we work on enabling policies and procedures to create respectful, inclusive and supportive environments. A key achievement was the development of our ‘Diabetes in the workplace’ resources for employers and employees to prevent workplace stigma and discrimination.
Common workplace issues we see include misconceptions about safety, assumptions about capability and some fear-based responses from employers, reinforcing the need for clear, accessible, stigma-reducing guidance.
During World Diabetes Day 2025, we invited workplaces to embrace the theme ‘Know more and do more for diabetes at work’ and used creative methods to engage on the messages.
Outcomes (achieved or expected)
The Diabetes Victoria strategic plan has a goal that ‘People will live free from diabetes stigma and discrimination.’ In 2024-25 the advocacy service contributed to this goal by supporting 1850 contacts, and we continue to work on new approaches to help all people affected by diabetes to feel respected in supportive environments.
Lessons Learned
We are aligning our workplace policy advocacy with emerging psychosocial hazard regulations, highlighting how stigma reduction contributes to psychologically safe workplaces.
We are also continually adapting our advocacy service to extend its impact on creating a more compassionate world for people with diabetes.

Alex Johnson, Diabetes Victoria
| Co-authors: | Joanne Walsh; Sandra Scalzo; Ruby O’Brien; Brittany Denton |
Background and Aims
Over the last two decades, Diabetes Victoria’s marketing campaigns have evolved significantly. Earlier Australian awareness campaigns, reviewed by the Australian Centre for Behavioural Research in Diabetes (ACBRD), were found to have limited impact on motivation and confidence, with 15% of viewers perceiving them as stigmatising. Fear-based messaging about diabetes often reinforced stigma.
This submission outlines Diabetes Victoria’s move toward empowerment-focused campaigns that are community-centred, promote understanding, reduce stigma and encourage action.
Methods
Diabetes Victoria now undertakes campaign development including:
Under this approach, people living with diabetes play a central role in ensuring campaigns reflect real experiences and promote understanding.
Outcomes
Diabetes Victoria has intentionally shifted from risk-focused campaigns toward messages centred on strength and lived experience. This is evidenced in campaigns such as recent Christmas Appeals, Tax Appeals, and the National Diabetes Week campaign: Check today for a healthier tomorrow (2025).
Outcomes include:
This model demonstrates how health organisations can move beyond fear-based messaging to build stigma-free, impactful campaigns.
Lessons Learned
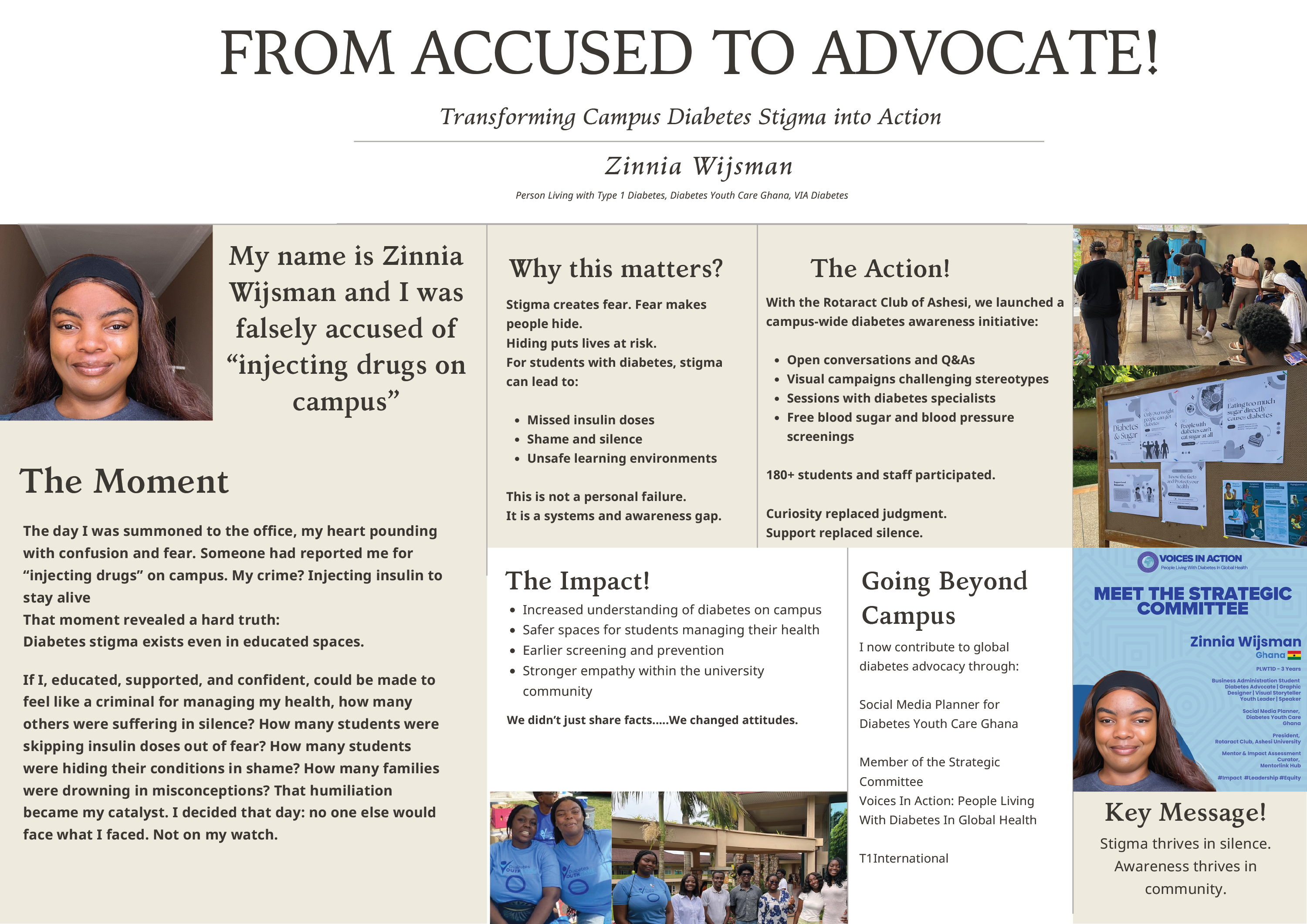
Zinnia Wijsman, Diabetes Youth Care
Abstract
I will never forget the day I was summoned out of class to the admissions office, my heart pounding with confusion and fear. Someone had reported me for “injecting drugs” on campus. My crime? Injecting insulin to stay alive.
As I sat across from administrators explaining that my insulin pen wasn’t paraphernalia, having to demonstrate myself pricking my finger to show that my condition was true, I felt shame burn through me, not for having diabetes but for being misunderstood in the one place I thought was safe. When they finally believed me, I didn’t feel relieved. I felt anger. And then, clarity.
If I, educated, supported, and confident, could be made to feel like a criminal for managing my health, how many others were suffering in silence? How many students were skipping insulin doses out of fear? How many students were hiding their conditions in shame? How many families were drowning in misconceptions? That humiliation became my catalyst. I decided that day: no one else would face what I faced. Not on my watch.
I began my advocacy journey with the help of a student-led organisation called the Rotaract Club of Ashesi, of which I am currently the President. We launched a campus-wide initiative to raise awareness about and promote diabetes screening. We didn’t just share facts; we shared humanity through interactive Q&As, open conversations, visual campaigns, amazing lessons from doctors specialized in diabetes, and free screening events, including blood sugar checks and blood pressure checks. Every word we chose honored the dignity of people living with diabetes. Every poster challenged stereotypes. Every screening became a safe space.
Over 150 students and staff attended, not just for the screening, but also to gain a deeper understanding of the topic. Strangers approached me, trying to understand more about diabetes, lecturers understood why I had to drink in class or why I could not make it, and students who once stared now asked, “How can I help?”
We didn’t just change minds. We changed hearts!
But I knew local actions needed global perspectives. I joined several organizations known for their advocacy on diabetes, such as Diabetes Youth Care in Ghana, T1International, and Voices In Action, immersing myself in the worldwide diabetes advocacy movement. I studied global trends, connected with advocates across continents, and helped amplify the voices of those still fighting for access, dignity, and survival. These organisations taught me that stigma has no borders, and neither should our fight against it.
Stigma thrives in silence. But one voice, which is rooted in pain, fueled by purpose, can shatter it. When we lead with vulnerability, we permit others to learn, grow, and care.
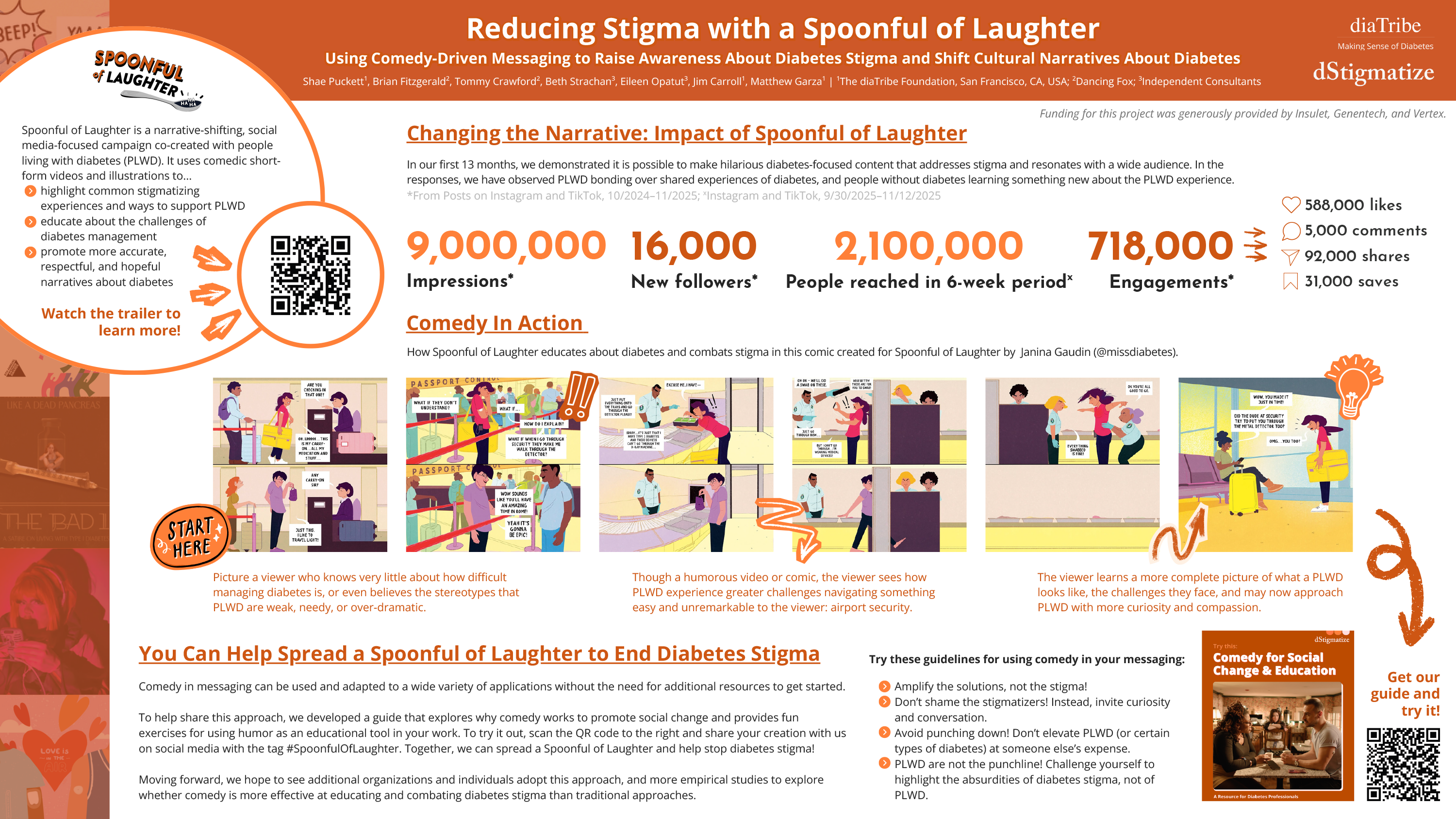
Amanda Puckett, The diaTribe Foundation
| Co-authors: | Brian Fitzgerald; Tommy Crawford; Beth Strachan; Eileen Opatut; Jim Carroll; Matthew Garza |
Abstract
Diabetes stigma is pervasive, impacting nearly 80% of adults living with diabetes. While research highlights methods such as language shifts and empathy-building exercises to reduce diabetes stigma, existing guidance is limited and focuses heavily on healthcare settings. To eliminate diabetes stigma, there is a need for broader awareness of the topic in the general public and effective strategies for reducing stigmatizing narratives and stereotypes about diabetes. As one potential solution, the diaTribe Foundation launched Spoonful of Laughter, a social media awareness and narrative-shifting campaign using comedy to educate about diabetes stigma while challenging harmful stereotypes.
The campaign used a combination of short-form video and illustrated comics, co-created with people living with diabetes (PLWD), to highlight common stigmatizing experiences, educate about challenges that PLWD navigate daily, and offer ways to support the diabetes community. Content was posted on Instagram and TikTok between October 2024 and November 2025, partnering with PLWD, nonprofits, and industry partners to amplify reach.
During the reported period, Spoonful of Laughter achieved over 9,000,000 views, 740,000 engagement actions (comments, likes, shares, and saves), and built a new audience of 16,000 people. The campaign’s reach peaked at 2,100,000 unique viewers in one 6-week window. Videos with the highest metric success had themes that both inspired relatability beyond the diabetes community while validating diabetes lived experiences.
These outcomes suggest that comedy-driven messaging can reach wide audiences both within and beyond the diabetes community and is useful for generating online discussion about life with diabetes and the impacts of stigma. The use of comedy-driven messaging on social media for awareness campaigns can be easily adopted by a variety of stakeholders with limited resources. Future research might explore the effectiveness of comedy-driven campaigns to increase issue awareness, reduce stigmatizing attitudes among audiences, and shift cultural narratives.

Amanda Puckett, The diaTribe Foundation
| Co-authors: | Diane Scherer; Chris Bright; Dessi Zaharieva; Matthew Garza |
Abstract
Physical activity (PA) has many benefits for people living with diabetes (PLWD), including improving glucose management and reducing risk factors for diabetes-related complications. However, research suggests that people experiencing diabetes or weight stigma may be more likely to self-exclude or be excluded from PA, thereby missing out on the potential benefits. Despite this, PA remains an underrepresented area in diabetes stigma research and education.
To address this gap, the diaTribe Foundation partnered with INSPIRE T1D, an international exercise and diabetes research collaborative, to conduct interviews with athletes with diabetes, advance awareness and understanding of the relationship between diabetes stigma and PA, and create resources to help healthcare professionals (HCPs), teachers, and coaches foster inclusive, stigma-free spaces for PLWD.
Semi-structured interviews with four young adult athletes living with T1D explored the barriers PWLD face to engaging with PA. Themes included stigma and lack of knowledge about diabetes among coaches and peers. We then developed two resources to address the barriers discussed by PLWD: one targeted at HCPs working with PLWD, and one targeted at coaches and trainers who may encounter athletes living with diabetes for the first time. These resources focused on the importance of PA for PLWD, essential information for fostering inclusive support systems for PA, and tips for having stigma-free conversations about PA. Four additional resources are in development to address additional subpopulations (such as T2D), and a marketing strategy is being developed to increase reach and awareness. We plan to measure impact with impressions, downloads, and direct outreach to HCPs and professional organizations representing coaches/trainers.
This work demonstrates a need for targeted education for HCPs and exercise professionals. Collaboration between researchers, advocates, and PWLD can catalyze the development of resources for reducing diabetes stigma in these environments.
Financial support for this study was provided by Novo Nordisk.

Kuan-yi Lin, Taiwan Association of Clinical Diabetes
| Co-authors: | Samuel Chen; Min-Ling Chen; Yau-Jiunn Lee |
Abstract
Despite Taiwan’s world-leading National Health Insurance system, diabetes stigma persists, creating structural barriers such as workplace exclusion, insurance denial, and regulatory lag (e.g., restrictions on Continuous Glucose Monitoring devices in national exams). In 2024, the Taiwan Association of Clinical Diabetes (TACD) launched the “End Diabetes Stigma” campaign. Following strategic collaboration with experts from the International Diabetes Federation (IDF) in Australia, the initiative pivoted from merely raising public awareness to implementing concrete, cross-sectoral policy advocacy.
By 2025, employing a multi-stakeholder strategy, the TACD achieved three major systemic breakthroughs. First, the publication of Taiwan’s first Physician-Patient Communication Guide aimed to refine medical language at its source. Second, hosting public hearings established a critical dialogue platform, successfully prompting the Ministry of Health and Welfare to commit to drafting CGM subsidies for Type 1 Diabetes patients, while legislators pledged to modernize medical device regulations to accommodate emerging technologies. Third, the signing of Memoranda of Understanding (MOUs) with corporations institutionalized supportive environments in the workplace. This case demonstrates that integrating a global perspective with local action can effectively transform destigmatization efforts into tangible policy reform, providing a practical framework for the global community.
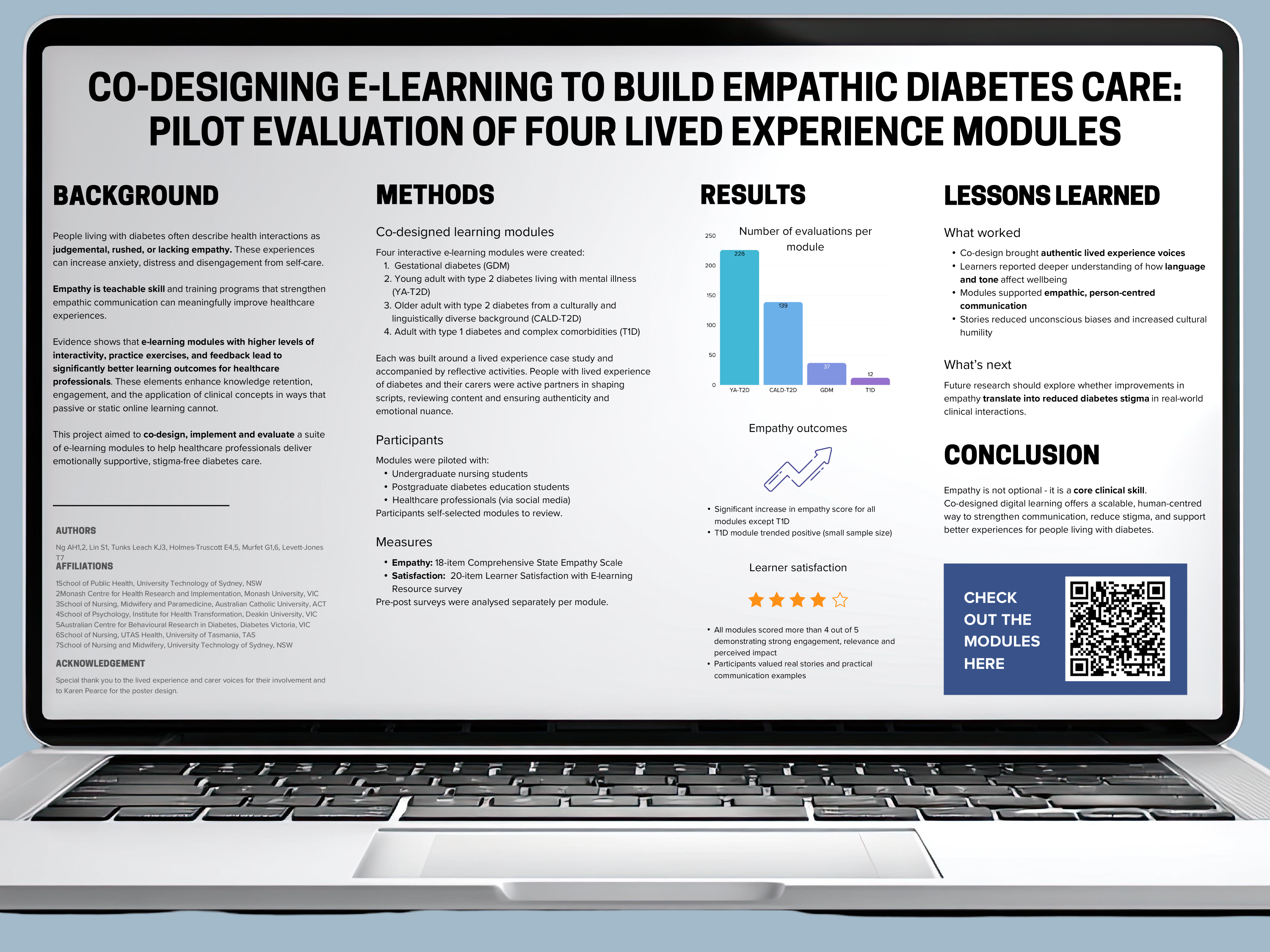
Ashley Ng, Monash Centre for Health Research & Implementation
| Co-authors: | Katie Tunks Leach; Elizabeth Holmes-Truscott; Giuliana Murfet; Tracy Levett-Jones |
Background
Stigmatising healthcare interactions are commonly reported by people with diabetes as lacking empathy, and contributing to anxiety, distress and reduced engagement in self-management. Empathic care is a teachable skill and essential for supporting people living with diabetes. This project aimed to co-design, implement and evaluate a set of e-learning resources to enhance healthcare professionals’ capacity to provide empathic care for people living with diabetes.
Methods
Four e-learning modules, including experiential video case studies and reflective activities, representing diverse experiences: woman with gestational diabetes (GDM); young adult with type 2 diabetes and mental illness (YA-T2D); older adult with T2D from a culturally and linguistically diverse background (CALD-T2D); adult with type 1 diabetes and complex comorbidities (T1D). Individuals with lived experience of these priority groups were invited to co-produce case studies. The modules were piloted with undergraduate nursing students, postgraduate diabetes education students, and healthcare professionals recruited through social media. Participants self-selected modules to review. Pre-post surveys assessed change in empathy levels (18-item Comprehensive State Empathy Scale; CSES) and learner satisfaction (20-item Learner Satisfaction with E-Learning Resource survey). Data were examined separately per module.
Outcomes
A total of 414 participants completed the pre-post surveys, with sample sizes varying per module (YA-T2D, n=226; CALD-T2D, n=139; GDM n=37; T1D n=12). Statistically significant improvements in empathy levels were observed for all modules except for that focused on T1D, which trended toward significance. Mean scores on the LSELR scale exceeded 4.0 on a 5-point scale, indicating positive learning experience from participants.
Lessons Learned
Co-designing case studies with people with lived experience provided authentic perspectives that enhanced understanding of the impact of language and behaviour in diabetes care. This approach supports empathic engagement and reduces unconscious burden. Future research should examine whether enhanced empathic care translates into measurable reductions in diabetes stigma within healthcare.
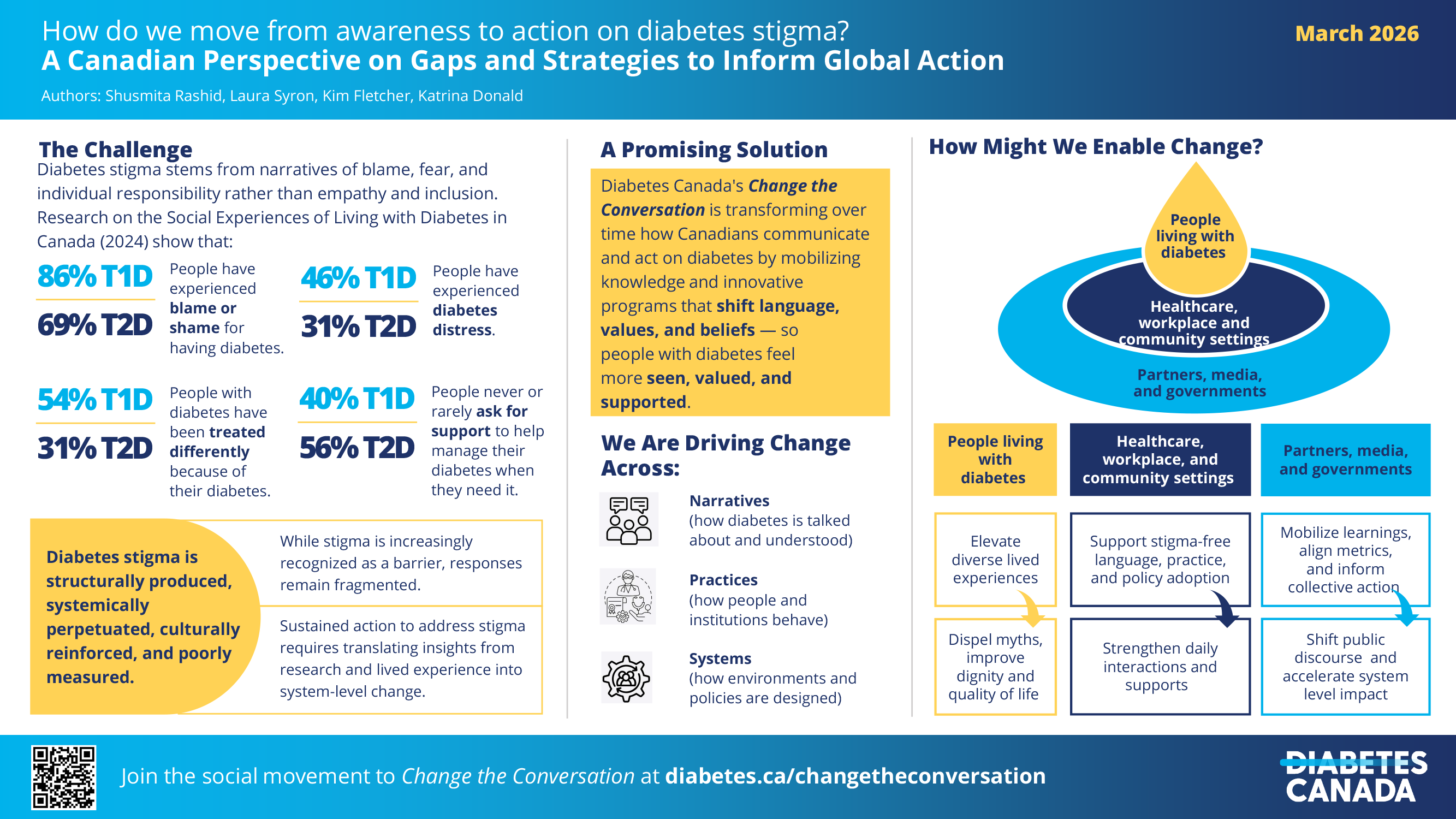
Shusmita Rashid, Diabetes Canada
| Co-authors: | Laura Syron; Kim Fletcher; Katrina Donald |
Background / Context
Diabetes stigma stems from narratives of blame, fear, and individual responsibility, rather than empathy and inclusion, where people with diabetes feel seen, valued and supported. Findings from Canada show that many people experience diabetes distress, stigma, and gaps in support that undermine health and quality of life [Diabetes Canada, 2024]. While stigma is increasingly recognized as a barrier, responses remain fragmented and uneven. Sustained action to solve this wicked problem requires translating insights from research and lived experience into system-level strategies.
Opportunities
Through Change the Conversation (CTC), Diabetes Canada designs and tests innovative approaches, including myth-busting campaigns, training, and other interventions aimed at fostering diabetes-inclusive spaces. These efforts exemplify the multi-level action required to change the language, beliefs, and values of and about people living with diabetes. Adapting these strategies across diverse contexts can accelerate progress toward a stigma-free future.
Challenges
Addressing diabetes stigma is challenging because it is structurally produced, systemically perpetuated, culturally reinforced, and poorly measured. Progress is hindered by the invisibility of stigma within national policies, the implicit bias among some healthcare professionals, self-blame among individuals, and structural stigma embedded in everyday systems. The lack of consistent measures to track progress at the individual, organizational, and system levels further complicates their implementation and scalability.
Recommendations
Elevate lived-experience storytelling to build awareness and empathy and motivate change in how people perceive and engage with people living with diabetes.
Build cross-sector alliances connecting healthcare, employers, and media for collective action.
Embed anti-stigma principles into healthcare, workplaces, and public systems to normalize inclusive practices.
Establish and share consistent metrics and strategies for mobilizing learning across local, national, and global efforts.
Meaningful Involvement of People with Lived Experience
People living with diabetes actively shape CTC, from assessing gaps and opportunities, to co-designing strategies to reflect real-world challenges and empower individuals and communities to lead change.

Alex St. John, Institut de recherches cliniques de Montréal (IRCM)
Background / Context
Strength athletes living with type 1 diabetes (T1D) often face unique challenges when intentional weight gain (a legitimate strength-building strategy) conflicts with medical assumptions about “good” diabetes management. While preparing for the historic Dinnie Stones lift in the Scottish Highlands, I strategically increased my body weight to build the strength needed for this feat. Rather than recognizing this as an informed evidence-based decision, my endocrinologist at the time dismissed my reasoning, pathologized the weight gain as “out of control”, and even suggested bariatric surgery (demonstrating how weight stigma and paternalistic care can override patient autonomy and expertise about their own bodies and goals).
Challenges
This experience reveals opportunities to train healthcare professionals in person-centred care that honours diverse life goals, athletic pursuits, and bodily autonomy. Strength sports communities can advocate for guidelines acknowledging legitimate reasons for weight management strategies beyond weight loss.
Challenges
Weight-centric care models and ingrained assumptions about diabetes management create barriers to truly individualized treatment. The intersection of diabetes stigma, weight bias, and gender in sport remained underexplored, particularly regarding who is believed and whose goals are validated.
Recommendations
Develop clinical competencies around athlete-centred diabetes care, create new or encourage participation in existing peer support networks connecting athletes with diabetes, establish protocols requiring healthcare professionals to understand patient goals before making weight-related recommendations, and amplify athlete voices in diabetes care guidelines.
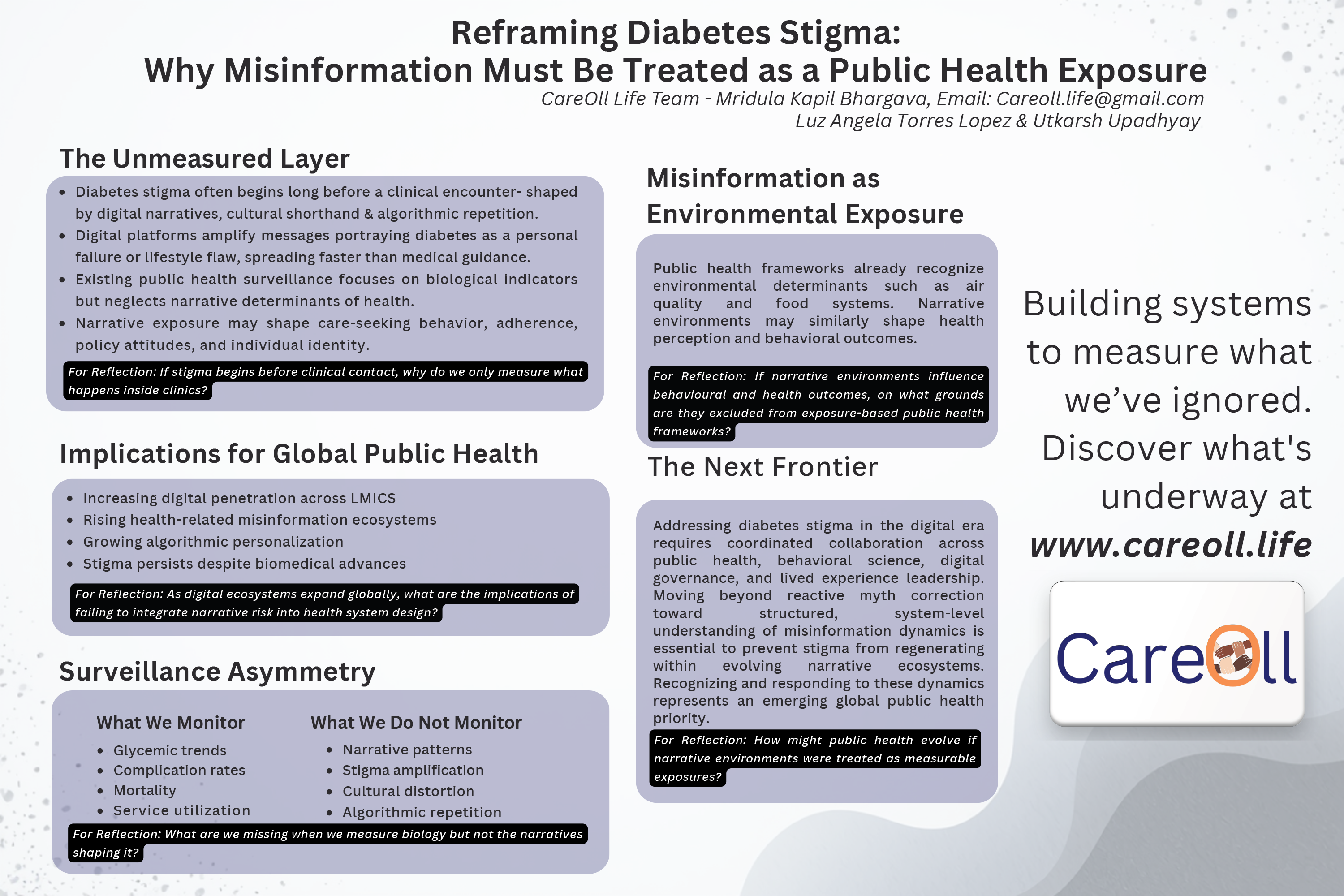
Mridula Bhargava, CareOll Life and Diabetes Fighters’ Trust
| Co-authors: | Dr Luz Angela Lopez, Utkarsh Udadhyay |
Abstract
Diabetes stigma is shaped long before clinical interaction. It forms when narratives portraying diabetes as a personal failure, lifestyle flaw, or reversible condition spread unchecked through digital channels, cultural beliefs, and commercial messaging. These messages circulate with emotional velocity, algorithmic amplification, and community repetition, often reaching individuals faster than credible medical guidance.
Despite global advancements in diabetes care, surveillance systems exist for glucose trends, complications, and biomedical outcomes but not for misinformation, which silently influences behaviour, policy attitudes, care access, and self-identity.
There is now a clear opportunity to treat misinformation as an analyzable and preventable phenomenon. With natural language processing (NLP), machine learning classifiers, sentiment analysis, and pattern-mapping tools, misinformation can be detected, categorized, and monitored the way we track epidemiological trends. This shift enables us to understand not just what misinformation exists, but also where it originates, how it evolves, and who it most affects.
CareOll- A Health Intelligence platform is being developed to establish this structured intelligence layer, combining real-time claim verification, AI-driven evidence retrieval, guideline mapping, and human-expert review. Beginning with diabetes and expanding gradually to other non-communicable diseases, the approach integrates technical rigor with compassion-based communication to avoid reinforcing shame or defensiveness.
Key challenges include multilingual processing, cultural interpretation, ethical content handling, and balancing precision with public accessibility. Opportunities lie in integrating this framework with advocacy, large scale research, locating the epicentre of misinformation and stigma, digital governance, health education, clinician support, and stigma-aware communication.
Reducing diabetes stigma requires more than correcting false statements- it requires building systems where truth becomes accessible, contextual, and trusted.
Meaningful Lived Experience Involvement
This work is led by an individual living with type 1 diabetes for 33 years and shaped through continuous consultation with people, families, NCD advocates and communities affected by stigma and misinformation. Their lived realities inform tone, priorities, usability, and direction.

Helga Nefdt, Ninety9Zero
| Co-authors: | Deeksha Dev |
Background / Context
Sexual well-being concerns are widely reported among women living with diabetes in both India and South Africa, yet remain largely absent in routine care. High prevalence of distress related to sexual function has been documented in women with Type 1 and Type 2 diabetes, impacting intimacy, self-esteem, and participation in care. However, cultural silence around sexuality and limited focus on women’s sexual health in diabetes practice result in significant unmet needs in both settings.
Challenges
Women in India describe feeling “undesirable” or “broken” due to fluctuating glucose levels, device visibility, and expectations related to femininity, marriage, and fertility. In South Africa, even when there is trust in healthcare, sexual well-being remains undiscussed due to limited training and the absence of structured screening practices in primary care consultations. Across both contexts, women frequently lack awareness that diabetes-related sexual concerns are valid and treatable. Internalized stigma, fear of judgment, and clinicians’ discomfort contribute to silence — not due to lack of need, but lack of safe openings for disclosure.
Recommendations
To support recognition and help seeking, three feasible approaches are identified:
Reflections
Sexual wellbeing is central to dignity and relationships and should not be treated as secondary to metabolic indicators. Routine, non-judgmental enquiry in India and South Africa can transform silence into agency — strengthening emotional safety and care engagement for women living with diabetes.

Archana Sarda, UDAAN An NGO for children with Diabetes
Background
Across the world, children with Type 1 Diabetes (T1D) survive not just because of strong systems, but because of strong communities. In low-resource settings, stigma—often around insulin—becomes the deepest wound: silence in families, shame in schools, gendered restrictions, curtailed livelihoods, myths around marriage and motherhood, and the quiet message that children with T1D are “lesser.”
UDAAN’s CHILD Model (Community-led Health through Integrated Localized Diabetes-care) emerged in rural India as a response to this pain. Twenty-five years ago, survival itself was rare. The model grew organically—from loss, listening, and the resilience of families who refused to abandon hope. Today, 80% of UDAAN’s team lives with T1D or has a child with T1D, making this approach deeply authentic and globally relevant.
As I often say:
“Stigma reduction begins when we walk our talk—when people with T1D hold a powerful place at every table of care, especially in the most resource-scarce settings.”
Opportunities (Grounded in UDAAN’s Successful Stigma-Reduction Work)
* Lived-experience trained educators and youth coaches who counter shame with credibility.
* School sensitization and structured youth advocacy by locals living with T1D that rewrite community perceptions.
* Local-language tools—animations, folk media, games, videos—that replace myths with understanding.
* 24×7 helplines and peer networks supporting families during stigma-triggering crises.
* Trained and structured support groups by local T1D moms, alongside adolescent clinics dismantling gendered stigma across the life course.
Challenges
Intersectional stigma remains invisible in formal metrics.
Funding undervalues lived-experience work.
Cultural norms still restrict autonomy.
Recommendations
* Recognize stigma reduction as a core clinical outcome.
* Institutionalize lived-experience advocates in diabetes programs.
* Track stigma indicators in registries: school retention, disclosure safety, gender outcomes.
* Build cross-sector partnerships to address culture, gender, and structural inequities.
* Adapt community-led models like CHILD by UDAAN across low-resource regions.

Emma Klatman, Life for a Child, Diabetes Australia
| Co-authors: | Frank Brennan; Alicia Jenkins; Graham Ogle |
Background / Context
Diabetes stigma and discrimination undermine dignity, constrain access to lifesaving care, and limit the ability of people living with diabetes to influence decisions affecting their own health. Our group previously undertook work examining rights-based advocacy, discrimination, and exclusion from participation through a human rights lens.
Opportunities
International human rights law provides a structured way to identify discriminatory or exclusionary practices, through elements of the right to health such as availability, accessibility, acceptability, quality, non-discrimination, and access to information. Two virtual rights-based workshops held in Africa (2021) and Latin America (2022) brought together people living with diabetes, families, clinicians, and human rights practitioners, including participation from the UN Special Rapporteur on the Right to Health. Participants described discrimination, marginalisation, information gaps, and limited influence over decisions affecting their care. A multilingual Diabetes Rights Toolkit was developed in response to lived experience realities to summarise human rights concepts raised in these discussions. This work was exploratory and intended to make legal ideas more accessible rather than prescribe specific solutions.
Challenges
The workshops and subsequent reflections highlighted how difficult it remains to translate rights-based principles into routine diabetes systems. Legal and human rights literacy is low across health systems; opportunities for people living with diabetes to influence decisions are often limited or symbolic; and structural inequities continue to shape exclusion, discrimination, and stigma. Interdisciplinary collaboration between diabetes stakeholders and human rights practitioners is still sporadic.
Recommendations
Future efforts should draw on established human rights standards within national diabetes strategies, strengthen legal and civic literacy among advocates and health professionals, and foster collaboration between those with lived experience, diabetes organisations, and human rights practitioners. Human rights mechanisms can help identify discriminatory practices and clarify state obligations, while stronger local advocacy infrastructures are essential for addressing system-level stigma and exclusion.
Meaningful Involvement
People living with diabetes contributed extensively to the workshops, raised the issues explored, and shaped the discussions and outcomes that informed this reflective work. These were early steps, and far more sustained lived experience leadership is needed for rights-based and stigma-related efforts to meaningfully uphold dignity and equality.
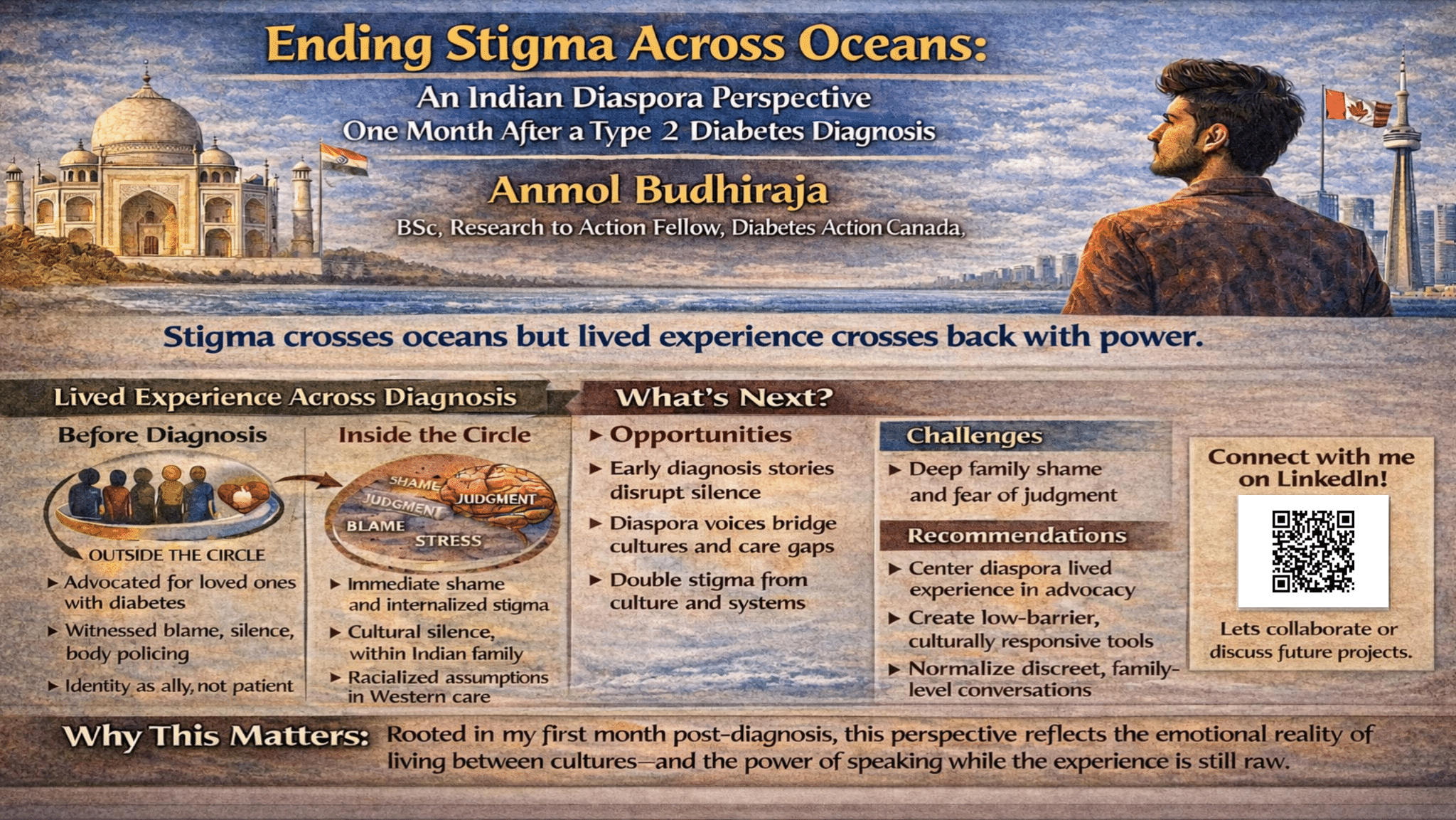
Anmol Budhiraja, Diabetes Action Canada (DAC)
Background / Context
I was diagnosed with type 2 diabetes only a month ago. In that short time, I’ve carried the familiar, heavy weight of shame rooted in memories of comments about my weight, unsolicited advice, and the expectation to remain “strong” and silent. As an Indian person who has lived in Canada for quite a long time, I now experience stigma from two directions: racialized assumptions in Western care and cultural stigma in my motherland that makes speaking about my diagnosis feel impossible. This dual burden places diaspora communities in a unique position to witness how stigma crosses borders, generations, and families.
Opportunities
Raw, early experiences of diagnosis can disrupt silence and challenge global stigma narratives. Diaspora experiences offer insights that blend cultural understanding with lived experience, revealing gaps in care and support. By sharing these stories, we can empower people who feel voiceless, inspire dialogue about stigma, and encourage culturally sensitive approaches in both Western and Indian contexts.
Challenges
Shame in Indian families, including my own extended families, silences people before they can even speak. Many suffer quietly rather than risk judgment or blame. Simultaneously, Western systems impose stereotypes that dismiss brown bodies. This double stigma traps individuals in fear, making the first months after diagnosis particularly isolating and emotionally complex.
Recommendations
Center diaspora lived experience in designing culturally sensitive advocacy and educational tools.
Provide low-barrier resources to empower people in the early months post-diagnosis.
Foster India–diaspora partnerships to tackle stigma with empathy and insight.
Normalize open conversations about diabetes within families using practical, accessible, and discreet advocacy tools.
Lived Experience Involvement
This perspective is rooted in my first month of diagnosis, shaped by my extended family’s silence, my cultural identity, and my work supporting others living with chronic conditions. It is informed by lived, loved, learned, and laboured experience, giving both urgency and authenticity to every insight shared.
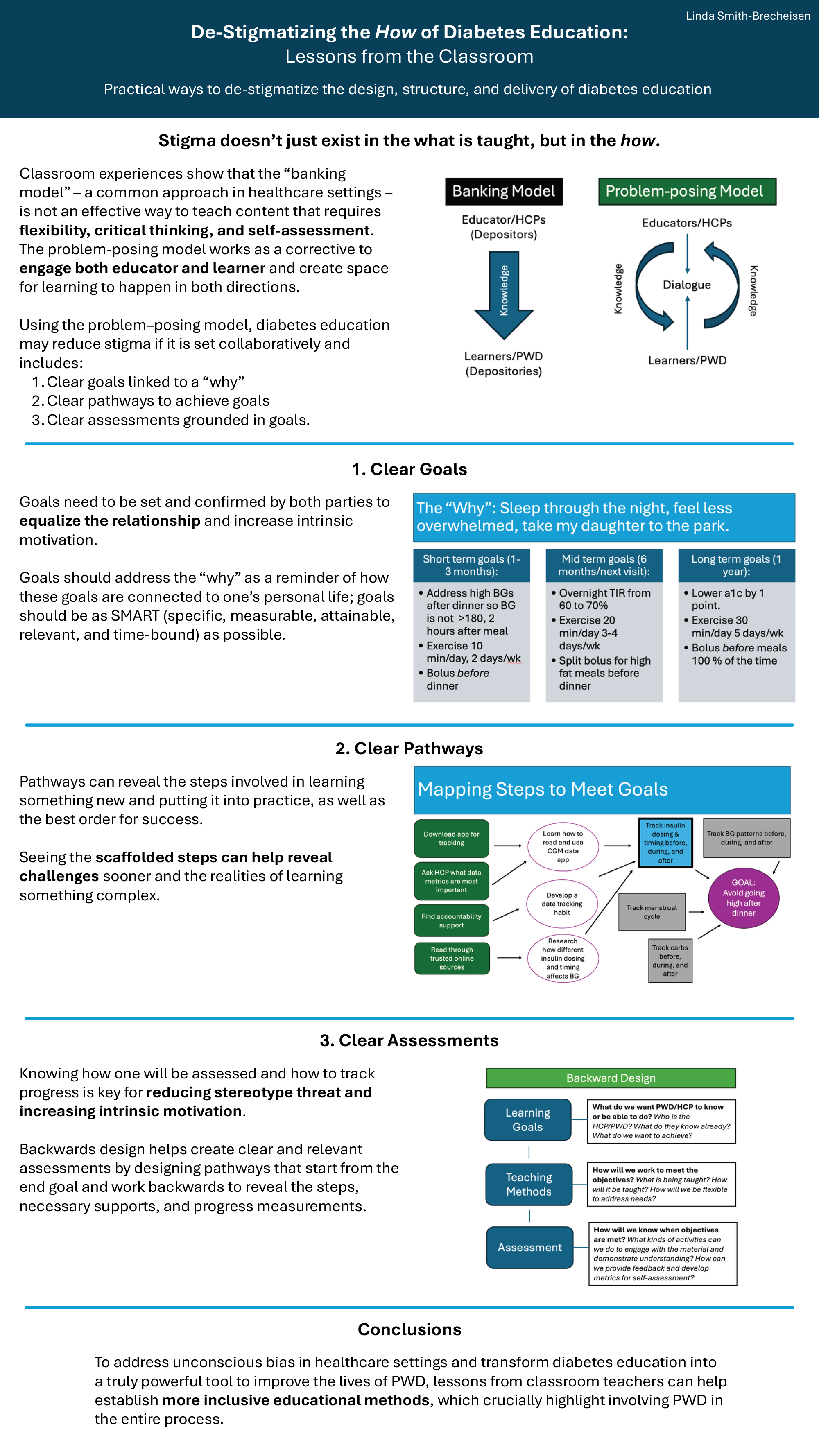
Linda Smith-Brecheisen, University of Texas at Dallas
Abstract
We know that stigmatizing language about diabetes has deleterious effects. What is less discussed is stigma that resides in another place: education. Stigma doesn’t just exist in the what is taught, but in the how. Discussions about stigma in diabetes have come a long way but have not yet addressed de-stigmatizing the design, structure, and delivery of diabetes education.
Data shows that people with diabetes (PWD) do not meet glycemic metrics set by healthcare providers (HCPs). Of the many interconnected issues, the target itself is problematic and the ways that PWD are eliminated from the decision making involved in creating assessment metrics and the pathways to achieve them. PWD are often demotivated because our lived experiences are rarely addressed or acknowledged as a form of expertise in our education and management and because the methods by which we are educated fail to address implicit bias built into the design.
To address bias in healthcare settings and transform diabetes education into a truly powerful tool to improve the lives of PWD, we must first understand the problems inherent in current diabetes education: How does current education design and delivery privilege some learners while punish others? How do biased HCP assumptions about PWD abilities impact learning outcomes?
We must then consult established inclusive educational methods, which crucially highlight involving PWD in the entire process: what can HCPs borrow from transformative and anti-racist educational design theories from foundational education scholars like John Dewey, who focuses on the value of experiential learning and Paolo Freire, who positions teachers and students as co-learners?
This talk will begin to open a much needed dialogue between HCPs and education experts who bring innovative ways of discussing and addressing stigma in education and who, crucially, involve students (in this case, PWD) to create more equitable outcomes.
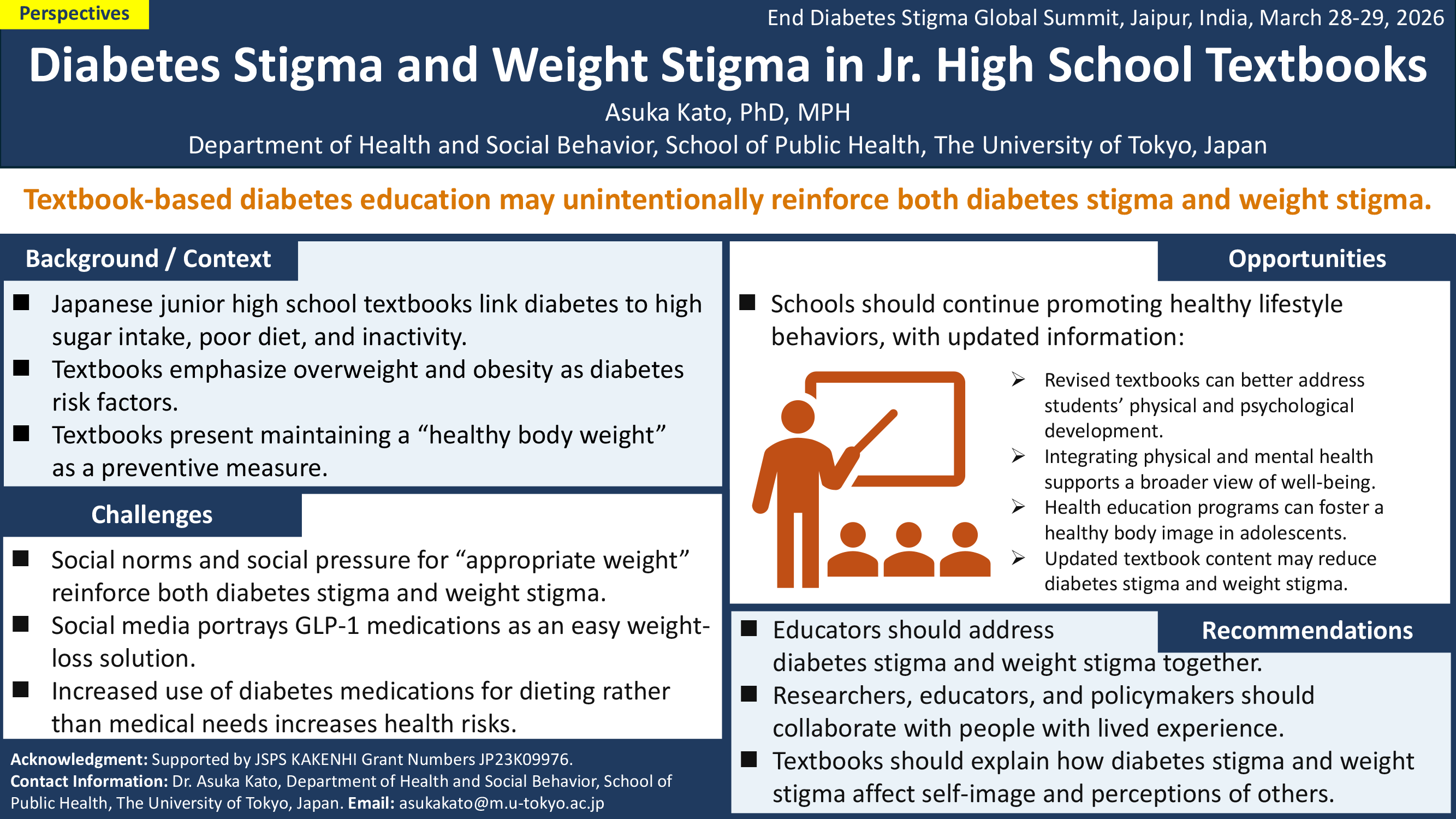
Asuka Kato, The University of Tokyo
Background / Context
In Japanese junior high schools’ health textbooks, diabetes is described as a condition caused by factors such as high sugar intake, an unbalanced diet, and lack of exercise. It is covered within units on healthy lifestyle habits, with warnings that being overweight or obese increases diabetes risk. Textbooks also emphasize the importance of maintaining a healthy body weight.
Opportunities
While schools should continue teaching the meaning of a “healthy lifestyle,” future textbook revisions need to better address students who are at a crucial stage of physical and psychological development. Integrating both aspects is essential for promoting a fuller understanding of “health,” reducing diabetes stigma and weight stigma, and helping students develop a healthy body image.
Challenges
A concerning trend has emerged among young people, particularly girls. Although the Japan Diabetes Society and the Japan Medical Association clearly state that the use of GLP-1 medications by individuals without diabetes is “off-label” and “inappropriate,” social media and online posts have spread appealing claims that these drugs suppress appetite and lead to weight loss without strict dieting or strenuous exercise. As a result, more young girls are purchasing GLP-1 medications originally intended for type 2 diabetes, using them for dieting or body image purposes rather than medical need.
Recommendations
In Japan, social pressure to maintain an “appropriate weight” or follow “proper weight management” has increased interest in medication-based approaches to weight loss, further driving demand for these drugs. These social norms also reinforce both weight stigma and diabetes stigma. Therefore, moving forward, working groups addressing weight stigma and diabetes stigma—together with individuals with lived experience of diabetes and obesity—should collaborate, as these stigmas are two sides of the same coin. Future textbook revisions must help students understand how these stigmas affect both themselves and others.
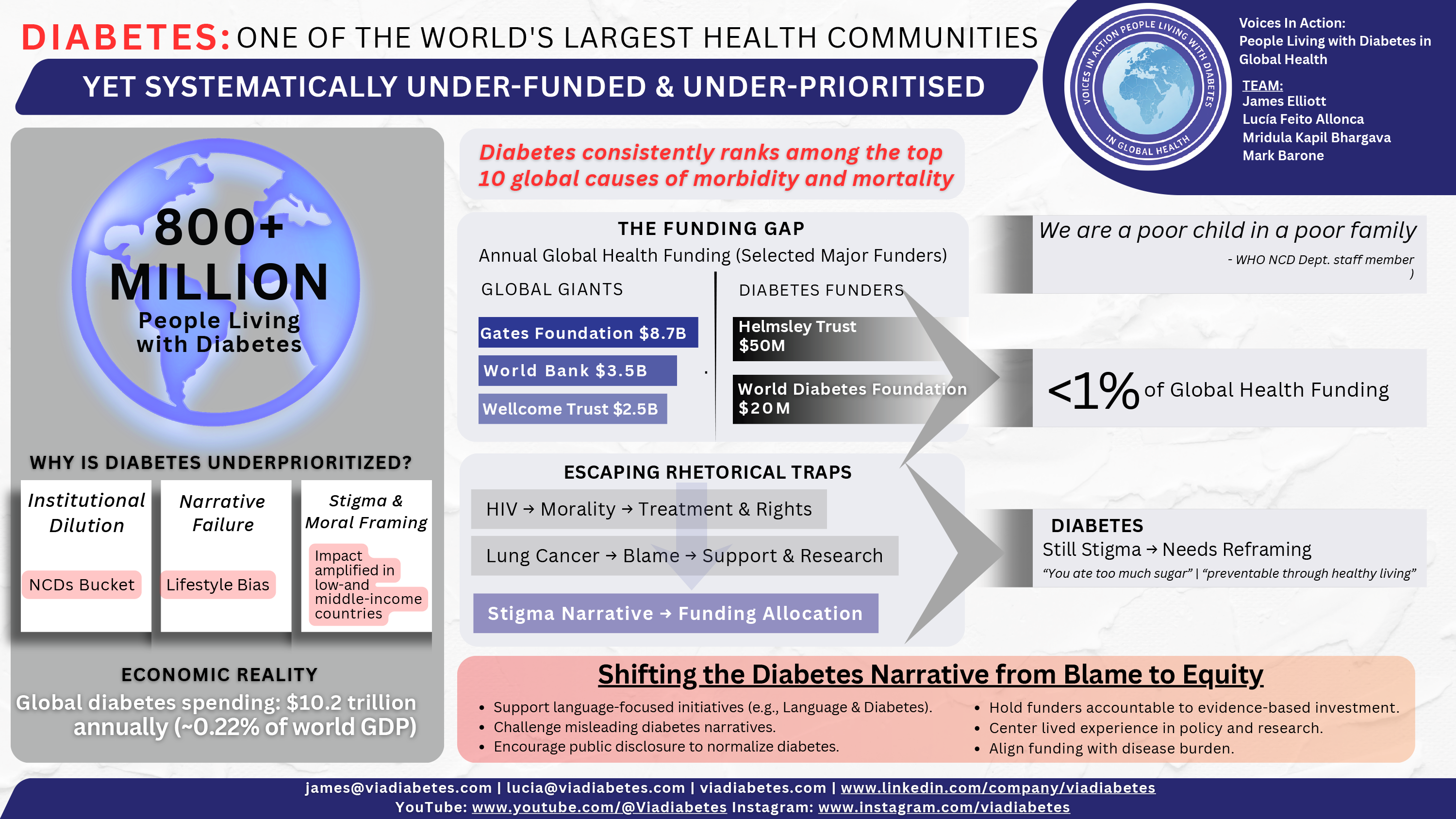
James Elliott, Voices in Action: PLWD in Global Health
| Co-authors: | Lucía Allonca; Mark Barone |
Abstract
Over 800 million people live with diabetes. This makes people living with diabetes one of the world’s largest condition-based communities. And yet, the amount of attention and resources given to diabetes pails in comparison to other health conditions, many that have just a fraction of the number of people affected. This segment will try and identify the reasons why there is such an imbalance.
Diabetes stigma will be examined as one of the causal factors of this imbalance between the impact of diabetes vs the limited amount of resources being dedicated to it. We will examine statements made by prominent global health actors, e.g., Gates Foundation, demonstrating their reluctance to fund diabetes related work.
We will also examine rhetorical traps global public health authorities are continuously falling into – and how we can help them escape. For example, diabetes is often portrayed as a condition one does to oneself. This leads to reductive narratives among the public like “you ate too much sugar” and causes uninformed policy-makers to have simplistic and inaccurate policy-fixes like “preventing and reverting diabetes, just involves diet and exercise”.
A similar dynamic existed for HIV and for lung cancer – yet these communities were able to break out of these rhetorical traps. We will use a scoping review and a series of key opinion leader interviews to examine how these communities achieved this.
The reluctance of key opinion leaders who live with diabetes to disclose their status will also be examined. The imprecise language used to describe diabetes will also be examined, for example not disclosing what type of diabetes is being discussed, the bundling of diabetes with conditions with different realities e.g., hypertension, obesity, cardiovascular disease. People living with diabetes and other chronic conditions are authors and will be meaningfully engaged in the process of creating this work.
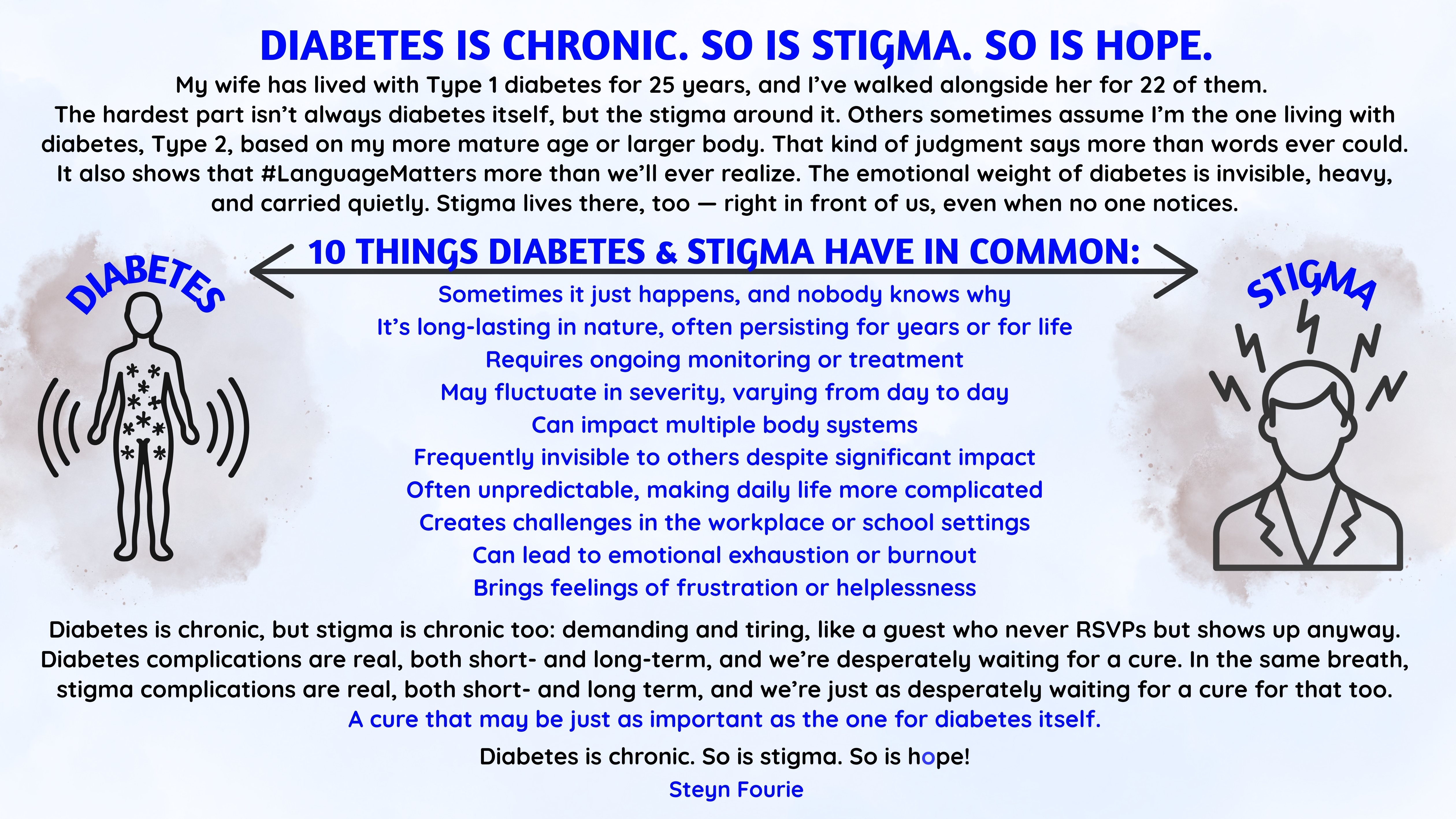
Steyn Fourie
Abstract
Creatively sharing my perspective on stigma and how it is a chronic condition in its own right.

Mark Thomaz Ugliara Barone, Intersectoral Forum of NCCs/NCDs in Brazil
| Co-authors: | Emma Klatman, Tinotenda Dzikiti, Sana Ajmal, Paul B. Madden |
Context
Stigma and discrimination related to diabetes affect daily life and shape how people living with diabetes are included in decision making about their care and support. Traditional stigma reduction often relies on information campaigns, yet structural change rarely happens without meaningful engagement and genuine social participation. When people living with diabetes help to shape policies, programs, and communication strategies, systems become more transparent, inclusive, and better aligned with real needs. Respectful and neutral language remains an important tool because it supports dignity and reduces blame, but language alone cannot transform environments where participation is restricted or symbolic.
Opportunities
Deepening meaningful engagement can help shift power imbalances that reinforce stigma. This includes integrating lived experience into advisory bodies, technology assessment, and policy consultations, valuing contributions as expertise. Social participation spaces, whether national councils, community groups, or global platforms, offer opportunities to co-design solutions, broaden public understanding, and challenge stereotypes. When communication guidelines are developed with people directly affected, language can better reflect inclusion and respect. #LanguageMatters and #NothingAboutUsWithoutUs must go hand in hand.
Challenges
Despite increased attention, many participation initiatives fall short. Barriers include unequal access to decision-making spaces, limited support for contributors, and practices that invite presence without influence. Stigma can also be embedded in institutional routines, shaping how priorities are set and which voices are heard. Without sustained commitment, engagement risks becoming procedural rather than transformative.
Recommendations
Meaningful Involvement of People with Lived Experience
All authors of this article are people living and working with diabetes. They contributed directly to framing the issues, identifying gaps, and shaping the recommendations summarized here. Their perspectives guided both the focus on participation and the understanding of how stigma is experienced in daily life, ensuring that proposed actions respond to real-world challenges.

Elia Nnko, Clinician & Type 1 Diabetes Advocate
Background/Context
Growing up in rural Tanzania, Type 1 diabetes was poorly understood. My parents believed insulin would cure me once the prescribed vials were finished, reflecting widespread myths and misconceptions about the condition. These beliefs shaped my early experience, introducing fear, secrecy, and uncertainty into daily life.
Challenges
Navigating a life-long condition in an environment where diabetes is misunderstood posed multiple challenges. Family hopes clashed with medical reality, and community advice often reinforced stigma rather than support. I learned to hide injections and mask symptoms to protect both my dignity and my family from social judgment. Even well-intentioned caregivers and relatives inadvertently contributed to misinformation.
Recommendations
From my dual perspective as a person living with Type 1 diabetes and as a clinician, I emphasize the importance of:
Reflections
These experiences highlighted that stigma often begins at home and within trusted networks. Addressing diabetes myths requires empathy, patience, and engagement with families as well as communities. By sharing my story and insights, I aim to provide a perspective that bridges personal experience and clinical understanding, emphasizing that compassion and knowledge are as vital as insulin itself in reducing stigma and supporting people living with diabetes.
Joanne Watson, Deakin University
Abstract
This paper argues that stigma in healthcare is not just prejudice but a structural failure of recognition, shaping who is seen as a person, who is deemed worthy, and who gets care. Drawing on Honneth’s Recognition Theory, I examine how misrecognition operates within health systems, influencing policy and practice and creating hierarchies of deservingness that ration healthcare resources.
Recognition Theory speaks to how individuals are categorised and whether they are acknowledged as members of groups deemed worthy of support. When recognition fails, people are positioned outside these categories, weakening their claims to care.
I write from two vantage points: as a speech pathologist and researcher working alongside people with intellectual and multiple disabilities, and as someone who has lived with diabetes for over three decades. Both groups, to varying degrees, experience stigma and misrecognition, where how they are categorised shapes their access to healthcare. Eligibility and resource allocation are often determined by categorical judgments rather than clinical need. These discrepancies can be further amplified by intersectional disadvantages such as culture, geography, socioeconomic status, and gender.
I argue for the relevance of conceptualising policy and practice with reference to Honneth’s theory of recognition and the urgent need to address misrecognition as a structural determinant of health. This call to action aligns with the End Diabetes Stigma movement, “encouraging initiatives, policies, and laws that promote equity,” not only for people with diabetes but as a model for ending stigma across all health systems.
Elizabeth Holmes-Truscott, ACBRD, Diabetes Victoria and Deakin University
| Co-authors: | Eloise Litterbach; Virginia Hagger; Renza Scibilia; Uffe Søholm; Timothy Skinner; Jane Speight |
Aims
Diabetes stigma is pervasive and harmful, yet evidence for effective stigma-reduction interventions remains limited. In 2021, Diabetes Australia released brief campaign videos advocating an ‘end to blame and shame’. This study explores: a) whether campaign videos are associated with diabetes stigma experiences (among adults with diabetes), endorsement (among adults without diabetes), or awareness (both cohorts); and b) perceptions of campaign videos (both cohorts).
Methods
Adults with diabetes (n=846: 42% T1D; 58% T2D; recruited via the National Diabetes Services Scheme) and without diabetes (n=1,397; via the Online Research Unit) took part in an online, three-arm randomised controlled cross-sectional study (1:1:1). Participants viewed stigma-awareness videos (intervention), alternate campaign videos (active control), or no videos (passive control). After, they completed measures of diabetes stigma experience (DSAS-1 / DSAS-2), endorsement and awareness (study-specific items). Mixed-methods feedback for intervention videos was also collected. Descriptive statistics and between-group comparisons were calculated, separately by cohort. A subset (n=290) of intervention-arm participants provided brief qualitative feedback which were thematically analysed.
Results
Intervention-arm participants reported greater experience (T2D only) and awareness (T2D; without diabetes) of diabetes stigma relative to controls (all p<.001; small effects). Across arms, a minority (<16%) of those without diabetes endorsed stigmatising attitudes. Campaign videos were positively rated as eliciting empathy (≥75% across cohorts), and described as being of educational value, personal resonance, and important for awareness-raising. Critiques included a lack of actionable solutions, over-exaggeration of diabetes stigma, and elicitation of pity. Some without diabetes reflected on campaign alignment with current attitudes or past behaviours
Conclusion
Findings support the role of diabetes organisations and communication campaigns in raising awareness of diabetes stigma among people without diabetes, and call for greater consideration of actionable solutions and avoidance of unintended consequences. Real-world evaluations of future campaigns are recommended.
Sarah Bradley, American Diabetes Association
Background
Weight stigma and bias within health care settings are pervasive worldwide and negatively affect clinical interactions, treatment engagement, and health outcomes for individuals with obesity. Although health system structures vary globally, stigmatizing language, clinical environments, and provider behaviors represent barriers to obesity care across countries and cultures. The 2025 Standards of Care in Overweight and Obesity emphasize the urgent need for clinician training, inclusive environments, and person-centered communication to reduce weight bias. In the United States, the ADA implemented an Obesity Stigma Training program across primary care settings to operationalize these recommendations and provide a model for translating stigma-reduction guidance into routine clinical practice.
Objective
To characterize the 2025 Standards of Care recommendations related to reducing weight stigma and to evaluate how a structured Obesity Stigma Training program enhanced provider awareness, confidence, and clinical behaviors, while identifying implementation elements with relevance for global adaptation across diverse healthcare systems.
Methods
Standards of Care recommendations were synthesized across three domains relevant to global obesity care: clinician education, clinical environment, and patient-centered communication. These domains were mapped to findings from a qualitative evaluation of the ADA Obesity Stigma Training, based on in-depth interviews with healthcare professionals (n=17) from nine primary care sites. The Consolidated Framework for Implementation Research (CFIR) guided analysis to assess intervention acceptability, contextual fit, and real-world application, highlighting implementation factors applicable beyond a single national context.
Results
The Standards call for multicomponent strategies to address implicit and explicit weight bias, which were reinforced through the training. Participants reported that the program:
• Increased recognition of unconscious bias and reframed obesity as a chronic, multifactorial disease rather than a personal failing.
• Improved communication practices, including greater use of empathetic, person-first language and permission-based discussion about weight.
• Heightened awareness of environmental inclusivity, prompting low-cost, scalable changes such as appropriate gown sizes, blood pressure cuffs, waiting-room seating, and exam-room preparation.
• Enhanced provider confidence when discussing weight, FDA-approved treatment options, and patient goals.
• Led to immediate and sustained changes in clinical behavior, improving patient comfort, engagement and willingness to return for follow-up care.
Sarah Bradley, American Diabetes Association
Background
Weight bias and stigma are pervasive across healthcare settings and contribute to significant disparities in care for individuals living with obesity. The 2025 Standards of Care in Overweight and Obesity consolidate evidence demonstrating that both explicit and implicit weight bias negatively influence physical health, psychological well-being, healthcare engagement, and treatment outcomes. Addressing these systemic and interpersonal forms of stigma is critical to improving the quality and equity of obesity care.
Objective
To summarize and translate the 2025 Standards of Care recommendations related to reducing weight bias and stigma in health care through clinician training, inclusive environments, and person-centered communication.
Methods
The 2025 Standards were reviewed with emphasis on the section addressing weight stigma and bias. Recommendations were synthesized across three domains: (1) education and training, (2) clinical environment and practice accommodations, and (3) communication and shared decision-making. Evidence supporting these recommendations—including systematic reviews, randomized trials, and qualitative research—was integrated to highlight rationale and expected impact.
Results
The Standards recommend early, continuous, and multicomponent training for all clinicians and staff to address the multifactorial etiology of obesity and reduce implicit and explicit bias. Evidence supports training approaches that combine didactics, empathy-building, self-reflection, and skills-practice, showing improved attitudes, increased empathy, and enhanced confidence in obesity care. The guidelines also specify environmental modifications—such as appropriate equipment, privacy during anthropometric measurements, and accessible waiting areas—to reduce stigmatizing triggers and improve patient comfort. Communication recommendations emphasize person-first language, avoidance of pejorative terminology, asking permission to discuss weight, and engaging in shared decision-making that prioritizes individualized, goal-aligned care.
Conclusions
The 2025 Standards offer a comprehensive, evidence-based framework for reducing weight stigma in health care. Implementing these recommendations across training, environment, and communication practices has the potential to improve patient experience, enhance trust, and support more equitable and effective obesity management.

Edwin B Fisher
| Co-authors: | Donna M Rice, Michele F Polz |
Background / Aim(s)
Mutual and peer support (MPS) are important for diabetes self management support. DiabetesSisters has planned, developed, and evaluated MPS may address stigma in its community (diabetessisters.org).1
Methods
DiabetesSisters is a community of women with diabetes providing intentionally varied resources for MPS through chats, meet-ups, webinars, online postings, coordinated through diabetessisters.org. Formative evaluation examined how members viewed stigma regarding diabetes, especially for women. Implementation of MPS addressed stigma, and impacts from surveys of DiabetesSisters showed benefits in reduced stigma.
Results
Formative evaluation — Key themes of stigma experienced by women with diabetes included:
• Fears about pregnancy, motherhood, and weight
• Social discomfort disclosing diagnosis at work or in personal relationships, especially among younger women
• Feelings of blame or shame related to diagnosis
• Misconceptions about the causes and management of diabetes
• Stigma linked to insulin use, device use, or diabetes-related complications.
Implementation included Meet-Ups (virtual as well as face-to-face) and topic-specific programming aimed at normalizing women’s experiences.
Implementation also included:
• Safe Spaces — Webinars and Meet-Ups provide judgment-free forums where women share stories and strategies for navigating stigma.
• Peer Narratives: Through articles and blogs, members discuss stigmatizing experiences and how they’ve confronted them.
• Targeted Education: MPS reframing internalized stigma with strength-based messaging.
• Focused Support: Dedicated opportunities for different ethnic groups and those with type 1, type 2, or gestational diabetes to ensure culturally relevant peer support where stigma may intersect with gender, race, and age.
Impacts: DiabetesSisters members report:
• Increased confidence in discussing their diabetes with others
• Reduced shame or embarrassment
• Greater sense of community and reduced isolation
• Reappraising negative societal messages about diabetes
Conclusion
DiabetesSisters has developed varied MPS features to address the ways in which women with diabetes experience stigma. Members of the community have recognized its value in these areas.
Description of how people with lived experience of diabetes are / have been meaningfully involved
In DiabetesSisters key chats, meet-ups and other activities center on sharing among women with diabetes and are developed with routine input from participants.

Michelle Hadjiconstantinou, University of Leicester
| Co-authors: | Jenny Hagan, Jane Speight, Melanie Davies |
Background
Early-onset type 2 diabetes (EOT2D; diagnosed <40 years) is increasing globally. Although diabetes-related stigma has been investigated in people with type 1 diabetes and type 2 diabetes (T2D), it remains understudied among adults with EOT2D.
Aim
Our aim was to explore experiences of diabetes-related stigma from the perspectives of adults with EOT2D and their healthcare professionals (HCPs).
Methods
This is a secondary qualitative analysis, including semi-structured interviews conducted with 25 adults with EOT2D and 25 HCPs. Data were analysed using reflexive thematic analysis, and presented using a stigma framework. Public contributors reviewed participant-facing documents and the interview questions.
Results
Findings from both adults with EOT2D and HCPs highlight drivers, experiences, and consequences of stigma in EOT2D, in addition to potential mitigating strategies. The media, HCPs, and others perpetuate stigma, driven by attitudes of blame from misconceptions that T2D is self-inflicted. Adults with EOT2D experience judgement and harmful stereotypes, including ‘unhealthy’, ‘lazy’, and intersectional stigma of ‘fat’ and T2D being an ‘old-persons disease’. Reported psychological consequences of stigma included embarrassment, self-stigma, and shame, leading to behavioural consequences of non-disclosure and reluctance to seek help. Education, awareness, and non-judgemental communication were highlighted as potential strategies to minimise diabetes-related stigma and consequences.
Conclusion
Stigma is highly pervasive in the lives of young adults with EOT2D, and can cause harmful consequences. Given the increased risk of physiological and psychological complications in this population, efforts to reduce stigma in EOT2D should be prioritised to encourage better care in younger adults. This is of importance when considering equity in diabetes care.

Sayli Jadhav, Independent Researcher
| Co-authors: | Chitra Selvan, Tejal Lathia, Meet Shinde |
Abstract
Research predicts that approximately 300 million people worldwide and 80 million in India would be living with Diabetes by 2026 with an increased number of young adults being diagnosed with Type 2 Diabetes (T2DM). Work on diabetes management highlights the facilitating role played by supportive human networks. Another trend emerging from psychosocial research on diabetes reveals persistent presence of experiences of stigma amongst people living with diabetes. Stigma researchers use quantitative tools to map the patterns of stigma and its emotional and psycho-social correlates; amongst which the impact on social relationships surfaces as most palpable. While research highlights the importance of high quality social relationships in managing diabetes; it also points towards the pervasive presence of stigma which could negatively impact these relationships. However, since quantitative methods merely demonstrate rather than explain associations and patterns, it becomes necessary for researchers to qualitatively explore the relational contexts of young adults living with T2DM in culturally situated ways.The current study aims to address this gap utilizing a grounded theory approach rooted in participant’s narratives of navigating their social relationships whilst living with T2DM. The participants of the ongoing study are 10 men and 10 women in the age range of 18-40 living with T2DM in urban India. The resultant grounded theory analysis seeks to espouse themes of relational manifestations of stigma in the psychosocial realities and support mechanisms of persons living with T2DM. Findings could help practitioners develop interventions that utilize patients’ relational contexts to promote better diabetes management and psychosocial wellbeing.
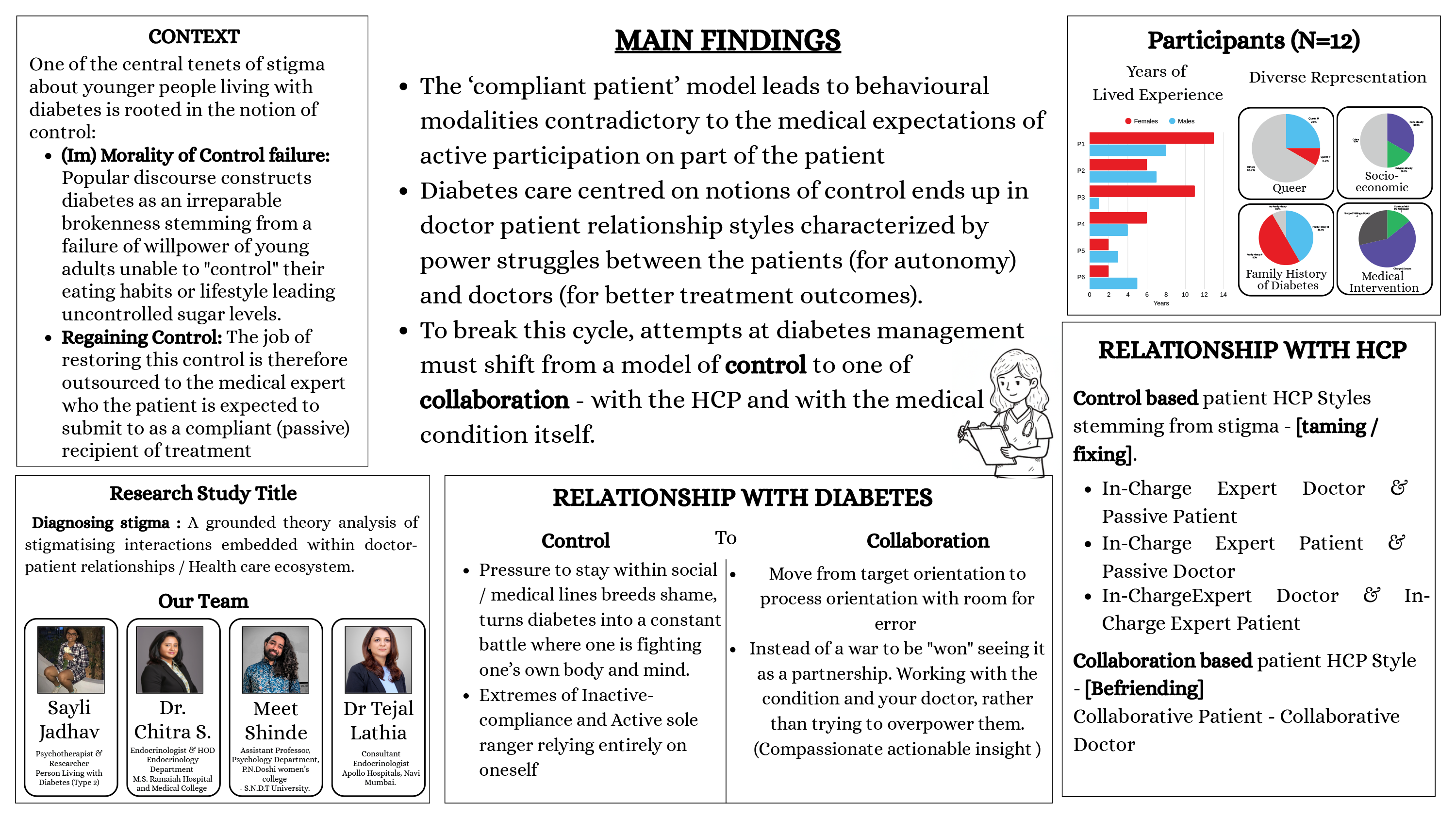
Sayli Jadhav, Independent Researcher
| Co-authors: | Meet Shinde, Chitra Selvan, Tejal Lathia |
Abstract
Diabetes related research spanning the last decade shows how Indians exhibit a higher genetic predisposition for diabetes and develop the condition at much lower body mass index (BMI) levels. The IDF Atlas predictions say that prevalence of Diabetes Mellitus (DM) in South East Asia will increase by 36% (from 9.7% to 13.2%) by 2050. Additionally reports indicate a reduced age of onset leading to a higher prevalence in young adult populations living with Type 2 DM. While a growing understanding on effective management of T2DM advocates for a strong doctor-patient relationship, research on barriers to health outcomes, point towards a hidden obstacle disrupting this dynamic – stigma. An Indian study by Vaz et.al reports that Medical and Nursing students attach more stigma to DM than the patients themselves, linking it to the medical condition along with socio economic background and other intersections of marginalization. Despite both, the alarming rise in the prevalence of diabetes amongst Indians and the potential impact of stigma, there is a significant gap in research dedicated to understanding specificities of diabetes stigma within the Indian context. This lack of understanding creates a significant knowledge gap, hindering the development of targeted interventions that address the specific cultural and social nuances surrounding diabetes in India. The current study attempts to address this gap, by employing a qualitative approach combining aspects of narrative inquiry and grounded theory. It utilizes in-depth interviews exploring nuances of the lived experiences of stigma amongst 20 young adults with T2DM. By delving into their experiences of diagnosis and treatment within the medical eco-system, the paper theorizes the specific manifestations of diabetes stigma in the Indian context of the doctor-patient relationship. The emergent themes could be utilised for developing interventions targeted at fostering an empathic and collaborative medical alliance.
Rajshri Mallabadi, SigmaMozak Solutions Pvt Ltd
| Co-authors: | Shweta Sharma |
Background
Stigmatizing language in diabetes care, such as blame-laden descriptions (“non-compliant,” “poor control”), weight-centered judgement, or directive, autonomy-limiting phrasing, negatively affects trust, engagement, and follow-up. Although global frameworks emphasize person-first, non-stigmatizing communication, routine clinical practice, and medical training rarely provide structured feedback to support behavior change.
Aims
This paper describes the development and early evaluation of ConversationAIly™, an AI-assisted tool designed to help clinicians and trainees recognize stigma-linked language patterns and adopt person-first, autonomy-supportive communication during simulated and supervised encounters.
Methods
ConversationAIly integrates Whisper-based speech transcription with a DistilBERT multi-label classifier trained on an annotated corpus of diabetes-care interactions. The model detects stigma constructs including moral judgement, negative framing, directive tone, and weight-based bias. Outputs include (i) identification of stigmatizing terms, (ii) discourse-level features such as question type and autonomy-supportiveness, and (iii) structured post-encounter feedback aligned with behavior-science frameworks (COM-B). Lexicons, annotation rubrics, and feedback categories were co-developed with clinicians and people with lived experience of diabetes. Preliminary testing included simulated consultations with clinicians and final-year medical trainees, as well as observational proof-of-concept studies in real-world outpatient settings.
Results
Across five proof-of-concept studies (N=125), patient-reported experience measures indicated high acceptability of person-first communication: 86% appreciated the language used, 93% reported willingness to continue their care journey, and 80% expressed satisfaction with consultation quality. Engagement indicators suggested better follow-up (76%), perceived treatment adherence (43%), and timely intensification (50%), though these findings were observational and not designed to infer causality. In a resident training cohort (n=20), the tool supported recognition of habitual stigma-linked phrasing and improved the consistency of faculty feedback. Deployment across programs training ~8,000 learners is informing iterative refinement of the educational framework.
Conclusion
Early findings support the feasibility and educational value of ConversationAIly™ as a structured tool for teaching and reinforcing person-first, non-stigmatizing communication in diabetes care.
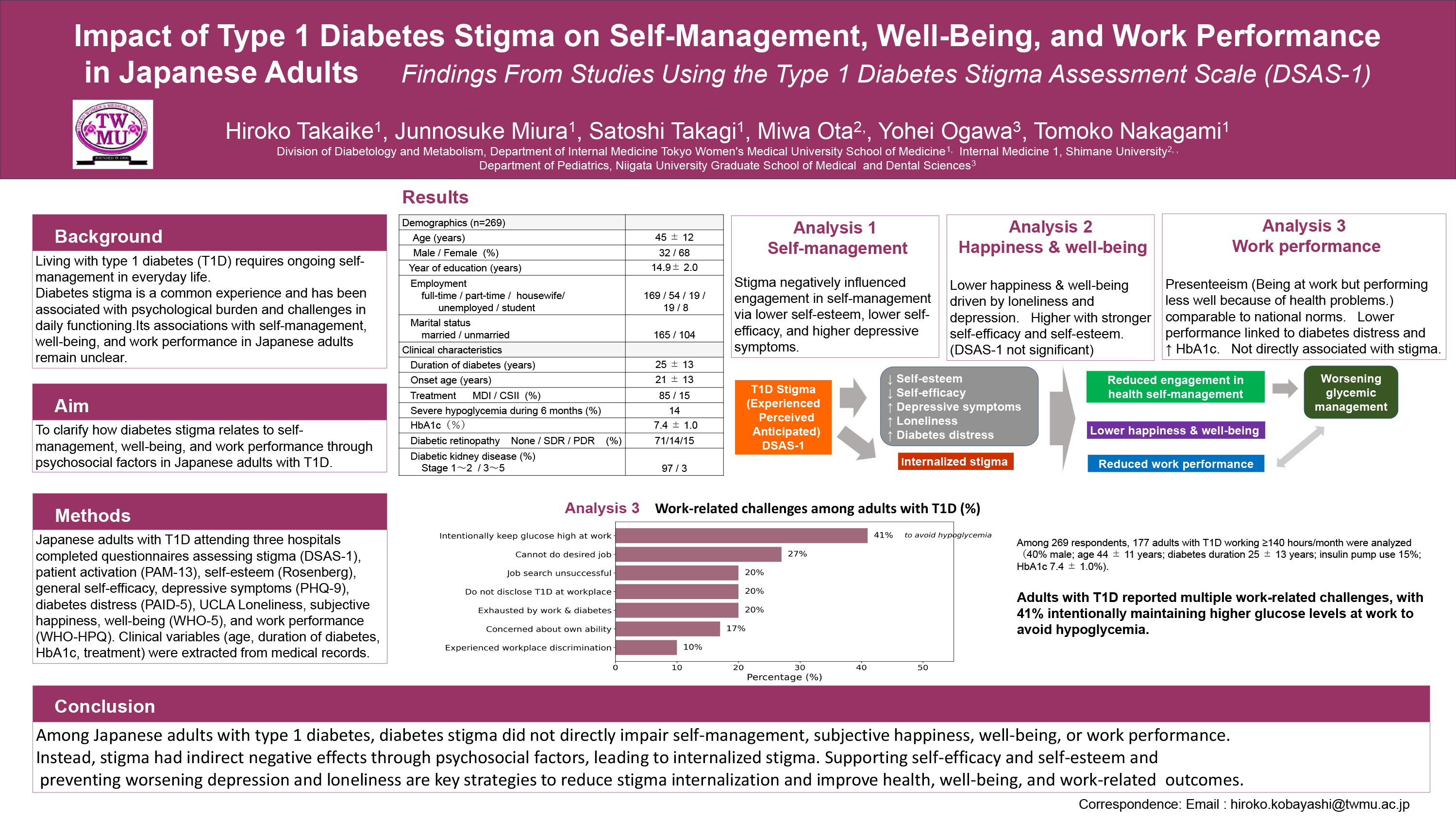
Hiroko Takaike, Tokyo Women’s Medical University
| Co-authors: | Junnosuke Miura; Satoshi Takagi; Miwa Ota; Yohei Ogawa; Tomoko Nakagami |
Background
Type 1 diabetes (T1D) requires continuous self-management behaviors, including frequent glucose monitoring and insulin administration. Stigma related to T1D—experienced, perceived, and anticipated—may hinder disease disclosure, limit self-management in public settings, and reduce social participation. However, the mechanisms through which stigma influences health management, well-being, and work performance have not been comprehensively examined in Japanese adults with T1D. We conducted a series of analyses using the Type 1 Diabetes Stigma Assessment Scale (DSAS-1) to clarify psychosocial pathways linking stigma to daily functioning.
Methods
Japanese adults with T1D attending three hospitals completed questionnaires assessing stigma (DSAS-1), patient activation (PAM-13), self-esteem (Rosenberg), general self-efficacy, depressive symptoms (PHQ-9), diabetes distress (PAID-5), subjective happiness, well-being (WHO-5), and work performance (WHO-HPQ). Clinical variables (age, duration of diabetes, HbA1c, therapy) were extracted from medical records. Structural equation modeling (Analysis 1) examined pathways from stigma to patient activation. Multiple regression analyses (Analysis 2) evaluated determinants of subjective happiness and well-being. WHO-HPQ scores were used to assess work performance and presenteeism (Analysis 3).
Results
We analyzed data from 269 adults with T1D (32% male; age 45 ± 12 years; diabetes duration 25 ± 13 years; insulin pump use 15%). Across analyses, stigma was positively correlated with diabetes distress, depressive symptoms, and loneliness, and negatively correlated with self-esteem, self-efficacy, happiness, and well-being. In Analysis 1, stigma did not directly reduce patient activation but exerted indirect effects through lower self-esteem and self-efficacy and higher depressive symptoms. In Analysis 2, subjective happiness and well-being were lower among individuals with greater loneliness and depressive symptoms and higher among those with stronger self-efficacy and self-esteem. In Analysis 3, absolute and relative presenteeism were comparable to national norms and unrelated to stigma; however, higher diabetes distress and elevated HbA1c were associated with lower work performance.
Conclusion
Among Japanese adults with T1D, stigma affects self-management engagement and well-being primarily through psychosocial mediators rather than direct effects. Many individuals struggle to balance work demands with glucose management, highlighting the need for more supportive and flexible workplace environments. Interventions targeting self-efficacy, self-esteem, loneliness, depressive symptoms, and diabetes distress could help prevent the internalization of stigma and support optimal health and work performance.

Matthew Larsen, University of Calgary
| Co-authors: | David Campbell |
Background
People with lived experience of homelessness and diabetes (PWLEHD) often experience intense feelings of shame due to their stigmatized conditions. Even though shame can cause numerous and significant adverse effects, no study has been done that specifically explores how or why PWLEHD feel and experience shame.
Objectives
The aim of our study was to understand the essence of the phenomenon of shame through exploring the experiences of PWLEHD.
Methods
We undertook a hermeneutic phenomenological study that involved 7 PWLEHD who were interviewed three separate times. Participants were questioned about their feelings of shame in regard to homelessness and diabetes. Interviews were transcribed verbatim and transcripts were analyzed using Interpretive Phenomenological Analysis. We also involved 5 community co-researchers from the Calgary Diabetes Advocacy Committee (CDAC), who participated in interview guide development, data gathering, and analysis.
Results
We found 4 main themes related to shame experienced by PWLEHD: shame in being vulnerable; shame in having to rely on inadequate support systems; shame in being isolated and lonely; and shame in experiencing profound and/or unexpected loss. Feelings of constrained agency permeated all 4 primary themes and was deemed to be the primary or essential element of shame for this population (Figure 1).
Conclusion
At a system level, any measures implemented that increase the agency of PWLEHD have the potential to reduce their shame. In addition, forming empathetic connections (especially with individuals with similar lived experience) can greatly mitigate the negative impact of shame for PWLEHD.

Michelle Hadjiconstantinou, University of Leicester
| Co-authors: | Ellen Hopwood; Clare Gillies; Sonia Khavere; Bernie Stribling; Kamlesh Khunti; Melanie Davies |
Background
Diabetes-related stigma is an important, often overlooked, social consequence of living with Type 2 Diabetes (T2D), with up to 70% of adults with T2D reporting experienced or perceived diabetes stigma. This refers to feelings or experiences of discrimination, negative attitudes, judgement or differential treatment, due to living with T2D. Despite growing recognition of diabetes-related stigma, previous systematic reviews have not integrated qualitative and quantitative evidence to comprehensively explore its impact on individuals living with T2D.
Aim
To explore the lived experiences of diabetes-related stigma in adults living with T2D, and its impact on clinical, behavioural, and psychological outcomes. Where available, evidence on stigma in the young population living with T2D (<40 years) will also be considered in comparison with older age groups.
Methods
MEDLINE, PsycINFO, CINAHL, the Cochrane Library and Scopus were searched from inception to August 2025 to identify eligible qualitative, quantitative and mixed-method studies on diabetes-related stigma in adults living with T2D. Two reviewers have independently screened studies and will appraise study quality.
Quantitative and qualitative synthesis will initially be conducted separately. Meta-analysis and subgroup analyses by geography, age, sex, ethnicity, and socioeconomic status will be performed where quantitative data allow. Thematic synthesis will be conducted to synthesise findings from qualitative studies. Where appropriate, qualitative and quantitative findings will be integrated to ascertain whether the findings support, contradict or add to each other.
Results
A total of 5,941 studies were identified from the database searches. Following title and abstract screening, 336 studies were sought for retrieval. Full text screening is nearly complete, with data extraction, quality appraisal and synthesis due to be complete January 2026.
Conclusion
These findings are expected to contribute meaningfully to research on diabetes stigma and support the development of evidence-based approaches and strategies to reduce T2D-related stigma.
Study Registration
PROSPERO registration number is CRD420251135305.

Laura Klinker, Research Institute Diabetes Academy Mergentheim
| Co-authors: | Andreas Schmitt; Eloise Litterbach; Elizabeth Holmes-Truscott; Jane Speight; Gina Lehmann; Dominic Ehrmann; Bernhard Kulzer; Norbert Hermanns |
Background
Eating patterns play a central role in glucose management across all types of diabetes and are often a focus of scrutiny. Qualitative research suggests eating patterns are a common marker of diabetes stigma. This study investigated the associations between diabetes stigma and unhealthy eating patterns among adults with type 1 (T1D) and type 2 diabetes (T2D).
Methods
In the PRO-Mental Study, adults with T1D and T2D recruited in secondary and tertiary healthcare centres in Germany completed an online survey, assessing diabetes-related eating problems via the Diabetes Eating Problem Survey-Revised (DEPS-R) developed for people with T1D and the general DEPS-10, and diabetes stigma (Diabetes Stigma Assessment Scales-1/-2: DSAS-1/-2), higher scores indicating more stigma and more eating problems. Blockwise linear regression was conducted by diabetes type, with DEPS-R(T1D)/DEPS-10(T2D) as dependent variable and all DSAS-1/-2 subscales as independent variables, adjusting for: sex, age, BMI, diabetes duration, GLP-1-medication.
Results
Of the 808 participants: 402 had T1D (♀53%, ♂47%, other 0.2%; mean+SD age 48±16years; diabetes duration 24±14years; DSAS-1 total: 37±14, DEPS-R: 11±9) and 391 had T2D (♀44%, ♂56%; age 63±11years; diabetes duration 15±10years; DSAS-2 total: 32±14, DEPS-10: 9±6). Among adults with T2D, higher DEPS-10 scores were most strongly associated with the DSAS subscales blame and judgement (ß=.27, p<.001) and self-stigma (ß=.21, p<.001), accounting for 17% explained variance beyond the significant contribution of higher BMI, younger age and GLP-1-medication. Among adults with T1D, higher DEPS-R scores were most strongly associated with blame and judgement (ß=.31, p<.001) and identity concerns (ß=.17, p=.002), explaining 14% additional variance to demographic factors.
Conclusion
This study shows significant associations between diabetes stigma and unhealthy eating patterns, particularly for the experience of blame/shame and internalisation of diabetes stigma (self-stigma and identity threat). Further research is needed to clarify causality, i.e. whether diabetes stigma contributes to unhealthy eating patterns or vice versa.

Firdous Shaikh, Jyoti and FRS Diabetes and Obesity Research Clinic
| Co-authors: | Kamran Khan; Riddhi Modi; Deeksha Dev |
Background and Aims
Diabetes-related distress encompasses the emotional and psychological challenges of living with diabetes, often compounded by stigma, isolation, and societal misperceptions. While clinical attention has traditionally focused on glycemic outcomes, the psychosocial burden—particularly stigma—remains inadequately addressed in routine care. Expressive art therapy, utilizing creative modalities such as painting, journaling, movement, storytelling, and music, offers a person-centered, non-judgmental approach to emotional wellness. This pilot study evaluated the impact of a multimodal expressive art therapy program on diabetes distress among individuals living with type 1 and type 2 diabetes, with particular emphasis on stigma reduction and global scalability.
Materials and Methods
This prospective, cross-sectional observational pilot enrolled 30 adults (aged 18–65 years) living with diabetes for >12 months, recruited from private diabetes clinics in Mumbai and Bihar. Two peer advocates living with type 1 diabetes co-facilitated the program, providing lived-experience perspectives that enriched participant engagement and created a safe, empowering environment. Diabetes distress was measured using the validated modified Diabetes Distress Scale (mDDS-20), published in the International Journal of Current Pharmaceutical Review and Research (Vol 17, Issue 10, Article 128). Participants independently engaged in ≥4 creative sessions weekly over 4 weeks, with optional weekend group support. Activities included emotion-themed painting, reflective journaling, culturally rooted dance/movement, narrative storytelling, and simple music-making—all self-paced and adaptable to diverse cultural contexts.
Results
Twenty-five participants (83.3%) completed the intervention. Mean mDDS-20 scores decreased significantly from 79.6±8.7 to 51.4±9.9 (35.4% reduction; p<0.001). Domains most improved: emotional burden (42%), social isolation (39%), and fear-related distress (30–34%). Qualitative feedback revealed that 89% felt “emotionally lighter,” 76% showed enhanced motivation for self-care, and 68% experienced improved diabetes-related communication. Peer advocates’ contributions were instrumental in fostering trust, normalizing experiences, and dismantling internalized stigma.
Conclusion
Expressive art therapy represents a low-cost, culturally adaptable, and stigma-reducing intervention with strong potential for global scalability. The integration of peer advocates living with diabetes enriches program effectiveness and authenticity. Further randomized controlled trials with diverse populations are warranted.

Sarah Manallack, Deakin University, School of Psychology
| Co-authors: | Jane Speight; Deborah Turnbull; Francois Pouwer; Elizabeth Holmes-Truscott |
Background
Adults with type 2 diabetes (T2D) report both diabetes and weight stigmas, however limited research explores differences in such stigma among subpopulations of adults with T2D, such as by age and/or gender.
Aim
To examine whether age and/or gender are independently associated with diabetes and/or weight stigmas among adults with T2D in Australia.
Method
Data were from the cross-sectional online Diabetes MILES-2 survey. Eligible participants (mainly recruited via NDSS) self-reported T2D. Validated measures assessed experienced and internalised diabetes stigma (DSAS-2 total score, subscales: blame and judgment; treated differently; self-stigma), and internalised weight stigma (WSSQ total score, subscales: fear of enacted stigma; self-devaluation). Across scales, higher scores indicate greater experience. (Un)Adjusted linear regression tested cross-sectional associations (confounders: BMI, diabetes-related complications, diabetes duration).
Participants
N=1,264; aged 61+9yrs (range 22-75); 43% women, 57% men; mean BMI 31+7kg/m2; 57% reported >1 diabetes-related complication/s; mean diabetes duration 11+7yrs.
Results
Age and gender together explained between 6-13% of the variance in DSAS-2 and WSSQ total and subscale scores (excluding WSSQ self-devaluation subscale). Across models, age was a stronger predictor than male gender (β<-0.32 vs β<-0.18). DSAS-2 scores were significantly lower for older participants (total, all subscales) and for men (total, blame and judgment subscale only); WSSQ scores were also significantly lower for older participants and men (total, fear of enacted stigma subscale only); range β=-0.1–β=-0.3. Observed independent associations were retained after adjusting for confounders, while higher BMI became the strongest predictor of higher WSSQ total and subscale scores (range β=+0.1–β=+0.3).
Conclusion
Results suggest differential experiences of diabetes and weight stigmas among adults with T2D; whereby younger adults and women more often reported such stigmas. This may suggest greater unmet needs relevant to their experiences. Qualitative exploration is needed to better understand lived experiences of subpopulations living with T2D.
Involvement of People With Lived Experience of Diabetes:
Item development for the DSAS-2 measure was informed by interviews with people with lived experience of type 2 diabetes. The DSAS-2 scale reduction and psychometric validation were informed via online surveys completed by people with lived experience of type 2 diabetes. For the Diabetes MILES survey, people with lived experience of type 1 and type 2 diabetes were asked what they wanted to see in a large-scale survey about living with diabetes in Australia. The survey was piloted among people with lived experience of type 1 and type 2 diabetes. Feedback was sought via interview, and survey adjustments made. While the Diabetes MILES data and the DSAS-2 development were informed by people with lived experience of diabetes, this study’s secondary analysis did not meaningfully involve people with lived experience of type 2 diabetes. We acknowledge this as a limitation of this study.

Siobhan Power, University College Dublin
| Co-authors: | Elizabeth Holmes-Truscott; Patrick Divilly; Francois Pouwer; Sonya Deschênes |
Aims
To examine the associations between diabetes stigma on general and diabetes-specific wellbeing, and to explore the moderating role of buffering and exacerbating psychosocial factors.
Methods
A cross-sectional survey was conducted with (n=289) adults living with Type 1 (T1D;n=117) and type 2 diabetes (T2D; n=189). More than half of the participants were female (n=157, 54%) and the mean age was 51 years (Range=18-86). Baseline characteristics were collected with validated questionnaires, including: Diabetes Stigma Assessment Scale 1 and 2; Patient Health Questionnaire-8; Generalized Anxiety Disorder-7; WHO5 Wellbeing Index, Adult Resilience Measure; Brief COPE, and Composite Weight Stigma Measure. Moderation analyses were performed using Process in SPSS, adjusting for age, gender, BMI, and education.
Results
Pearson correlations revealed that diabetes stigma was significantly associated with poorer mental health (depression, anxiety) and greater diabetes-specific psychological distress (i.e., diabetes distress) in both T1D and T2D. Moderation analyses revealed that resilience weakened the association between stigma and anxiety in T1D (p<. 05,β=-.008). In T2D, weight stigma strengthened the association between diabetes stigma and depression (p<. 05,β =.036), and avoidant coping strengthened the association between diabetes stigma and anxiety (p<. 05,β =.009). Avoidant coping weakened the link between diabetes stigma and wellbeing in T1D (p<.05,β =.130), suggesting a potential protective effect under certain conditions.
Conclusion
These findings highlight the complex interplay between diabetes stigma, psychosocial factors, and mental health outcomes. Potential areas for intervention may include approaches that not only reduce stigma but also enhance resilience, while addressing weight stigma and avoidant coping.

Debby Syahru Romadlon, Chulalongkorn University
| Co-authors: | Rudy Kurniawan; Safiruddin Al Baqi; Mario Pratama |
Background and Aims
Stigma related to type 2 diabetes is a key psychosocial barrier that undermines self-management and worsens health outcomes. However, culturally validated stigma measures remain scarce in many non-Western contexts. This study aimed to culturally adapt and psychometrically evaluate the Indonesian Version of the Type 2 Diabetes Stigma Assessment Scale (I-DSAS-2) for adults with type 2 diabetes in Indonesia and to examine its relationships with A1C, fatigue, and depressive symptoms.
Methods
A cross-sectional psychometric and correlational study was conducted with 190 adults attending outpatient clinics. The DSAS-2 was translated and culturally adapted using standardized procedures. Psychometric testing included exploratory factor analysis, internal consistency (Cronbach’s alpha), and test–retest reliability (intraclass correlation coefficient, ICC). Clinical outcomes were assessed using A1C, the Indonesian Multidimensional Fatigue Inventory (IMFI-20), and the Beck Depression Inventory–II (BDI-II). Associations between stigma and clinical variables were examined with Pearson correlations and multiple linear regression, controlling for age, sex, diabetes duration, and comorbidities.
Results
The I-DSAS-2 demonstrated strong psychometric properties, yielding a three-factor structure (treated differently, blame and judgment, and self-stigma), high internal consistency, and strong test–retest reliability (Table 1). Higher stigma scores were significantly associated with poorer glycemic control (higher A1C), greater fatigue, and more severe depressive symptoms. In adjusted models, stigma remained an independent predictor of all three outcomes, with the strongest association observed for depression (Table 2).
Conclusion
The I-DSAS-2 is a valid, reliable, and culturally relevant instrument for assessing diabetes-related stigma in Indonesian adults and underscores its multidimensional nature and strong links with key clinical outcomes.

Chris Bright, University of Worcester
| Co-authors: | Győző Molnar |
Abstract
Diabetes has become a condition which is acknowledged for its global impact on healthcare and society. However, much of sport research has followed a physiology- focus that has increased awareness of the condition’s effect on the body with a limited understanding around its socio-cultural consequences. This chapter fills this gap by exploring the identity conflict that footballers with Type 1 Diabetes (T1D) experience. Six male T1D football players were recruited and interviewed. Data were captured utilising a netnographic approach. The data were then put to a narrative thematic analysis. Participants demonstrated that athletic identity and elitism in sport adversely impacts their identification with T1D. The data also revealed that the social-relational model of disability’s connection with identity is the closest replication of identity negotiation between disability, T1D and participants. Stigma surrounding T1D was shown to have a significant impact on reducing identification with the condition, which was also linked to behaviour that negated medical advice and adherence to it. The Neo-Tribe concept offers an explanatory framework as to how identity conflict was negotiated through the temporary identification with T1D and the positive lever of football, driving an increased uptake in peer support and subsequent medical adherence.
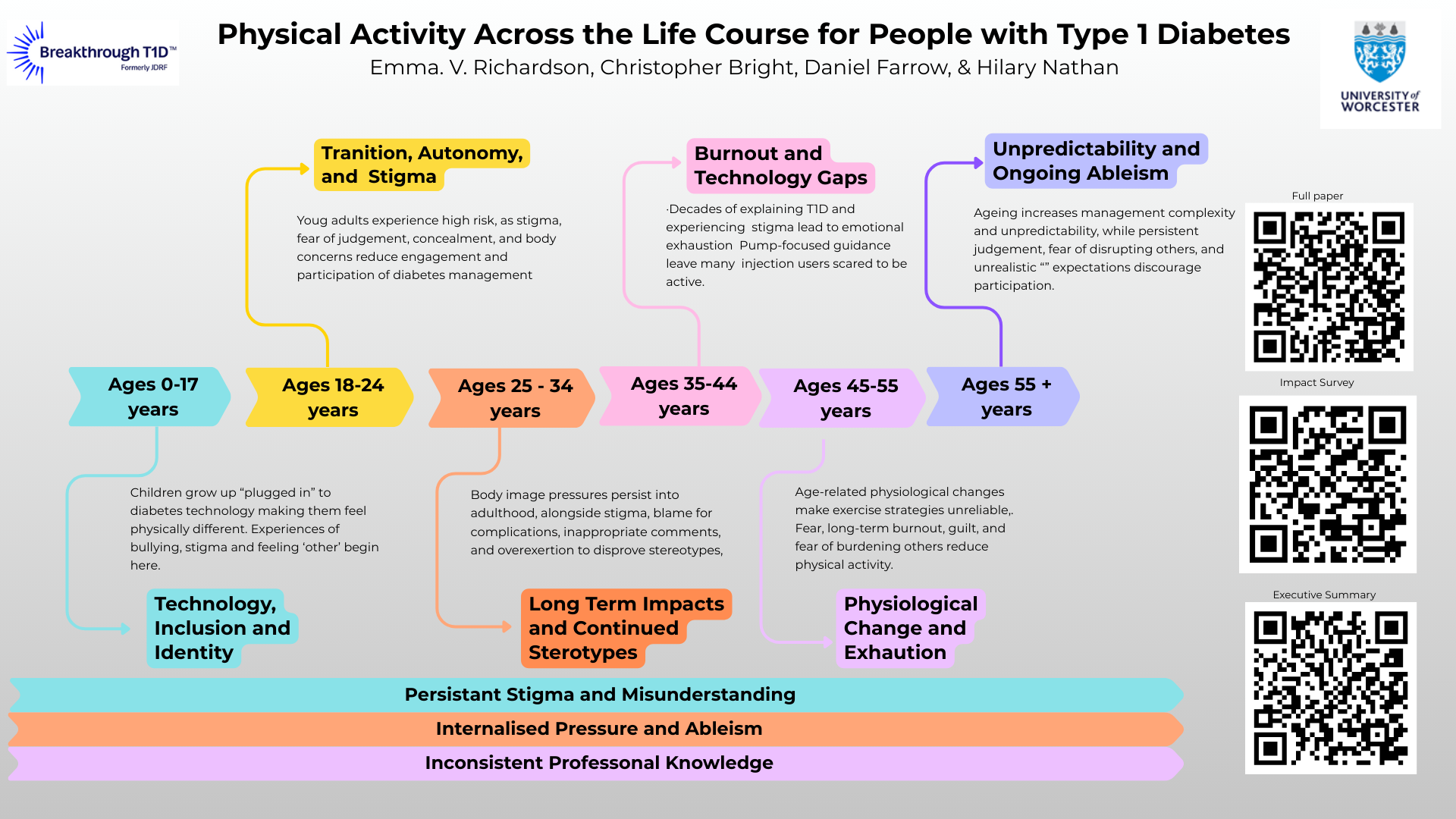
Emma Richardson, University of Worcester
| Co-authors: | Christopher Bright; Daniel Farrow; Hilary Nathan |
Abstract
People living with Type 1 Diabetes (T1D) encounter complex and often marginalised relationships with physical activity (PA) across the life course. Drawing on qualitative responses from 311 participants aged 3–75 years in the United Kingdom (UK), this study explored how stigma, internalised ableism, and sociocultural narratives shaped PA experiences for people with T1D. Using reflexive thematic analysis, we examined age-based case studies to understand how PA becomes meaningful—and, at times, fraught—at different life stages. Findings reveal that stigma is not episodic but accumulative. From childhood, participants faced ableist assumptions, exclusionary practices in schools and sports clubs, and misunderstandings from educators and peers about T1D management. These early interactions fostered shame, hypervigilance, and identity negotiations around visibility of devices such as insulin pumps and continuous glucose monitors. In adolescence and young adulthood, the desire to “feel normal” intersected with stigma related to body image, public glucose monitoring, and misconceptions about dietary needs. For many, these experiences contributed to internalised ableism and, in some cases, disordered eating or avoidance of PA environments. Across adulthood, participants described persistent stereotyping, intrusive commentary, and social policing of their self-management practices. By midlife and older age, decades of stigma contributed to “comment burnout,” emotional exhaustion, and reduced motivation to engage in PA despite strong health incentives. The interplay of changing physiology, technological expectations, and ongoing scrutiny reinforced feelings of inadequacy and burden, underscoring how ableist norms and neoliberal health discourses shape PA participation. This study highlights a critical need for disability-inclusive approaches to PA that go beyond biomedical guidance. We call for structural, policy, and cultural change that challenges ableist assumptions, improves practitioner training, and centres lived experience. Supporting equitable PA across the life course requires acknowledging stigma not as an individual challenge but as a systemic.

Emmanuel Ekpor, Deakin University
| Co-authors: | Sarah Manallack; Matthew Garza; Jane Speight; Elizabeth Holmes-Truscott |
Background/Aims
The international consensus on diabetes stigma highlights the urgent need to address stigma in healthcare. This systematic review synthesised qualitative evidence to provide comprehensive, context-specific insights into how type 2 diabetes (T2D) stigma operates in healthcare settings, with the future goal of informing stigma-reduction interventions and guidance.
Methods
We performed a systematic search on PubMed, CINAHL, and PsycINFO (from inception to April 2025), supplemented by forward/backward citation tracking. Studies were included if they reported qualitative data on T2D stigma within healthcare settings, from the perspectives of people with T2D and/or healthcare professionals (HCPs). Data were analysed thematically using a hybrid deductive–inductive coding approach. Deductive coding was guided by the Health Stigma and Discrimination Framework (HSDF), examining four key domains of stigma: manifestations, drivers/facilitators, markers, and impacts.
Findings
We identified 46 eligible articles (k=7 including HCPs only, k=28 people with T2D only, and k=11 mixed sample; N=1,972; 26 countries). All HSDF domains were evident. Individuals with T2D perceived, experienced, anticipated, and internalised T2D stigma, perpetuated through HCPs’ communication, attitudes, and practices. T2D stigma was driven by stereotypes, authoritarianism, and lack of knowledge; and facilitated by overly simplistic models of care and healthcare-related media misrepresentation. Impacts spanned psychological well-being, health-seeking behaviours, quality of care, and interpersonal relationships with HCPs. People with T2D called for HCPs and system-level reforms to foster stigma-free T2D healthcare.
Conclusion
These findings strengthen understanding of T2D stigma in healthcare, showing how pervasive it is, with significant consequences for people with T2D. They reveal actionable drivers and facilitators, which can be used to develop targeted interventions and guidance towards stigma-free T2D care.
Chasia Lewis
Introduction
Type one diabetes is a chronic condition characterized by the inability of the pancreas not to produce insulin due to the autoimmune destruction of the beta cells in the pancreas. It is often diagnosed in kids and young adults.
Objective/Purpose
The main purpose of this paper is to bring an overview of the life of a Type one diabetes champion in managing this condition. It also sights the major challenges experienced by the diabetes champion during their lifetime with diabetes.
Method
This research was carried out through physical engagement with the diabetes champions where they shared their stories outlining the major setbacks during they face. Questionnaires too were administered to them where I got their sentiments.
Body
Living with Type one diabetes in a low-income country like Kenya has proven to be a very hectic and cumbersome task especially in the proper management of the condition. Many young adults are perishing due to the horrors of diabetes complications such as DKA, diabetic wounds, dialysis and depression due to amputations and the rough economic times. The inadequate amount of insulin in Kenya has posed a major problem among diabetes patients where due to the inability to afford the insulin, many end up dying and developing diabetes complications.
The paper also highlights the challenge of insulin storage, where many patients lack refrigerators where they can safely store their insulin. Thus, as a result of due to poor storage, many patients end up using ‘faulty insulin’ due to loss of potency hence death. Accessing diabetes glucometers and glucostrips is another setback since they are extremely expensive and many of the lack in the Third world market. The text also sights the social problems faced by kids and young adults in managing this condition. Due to insufficient diabetes education and awareness in Kenya, many kids and young adults face a lot of stigmatization due to discrimination both in schools and public places. This has culminated and has brought huge concerns about diabetes and relationships. Many young adults with diabetes suffer due mental stress as a result of issues brought about by diabetes in finding a partner to have a relationship with.
Conclusion
Living with Type one diabetes in Kenya is evident that it is cumbersome though by having access to insulin and diabetes products such as glucometers and test strips, proper management can be achieved and hence increase the quality of life among diabetes patients.
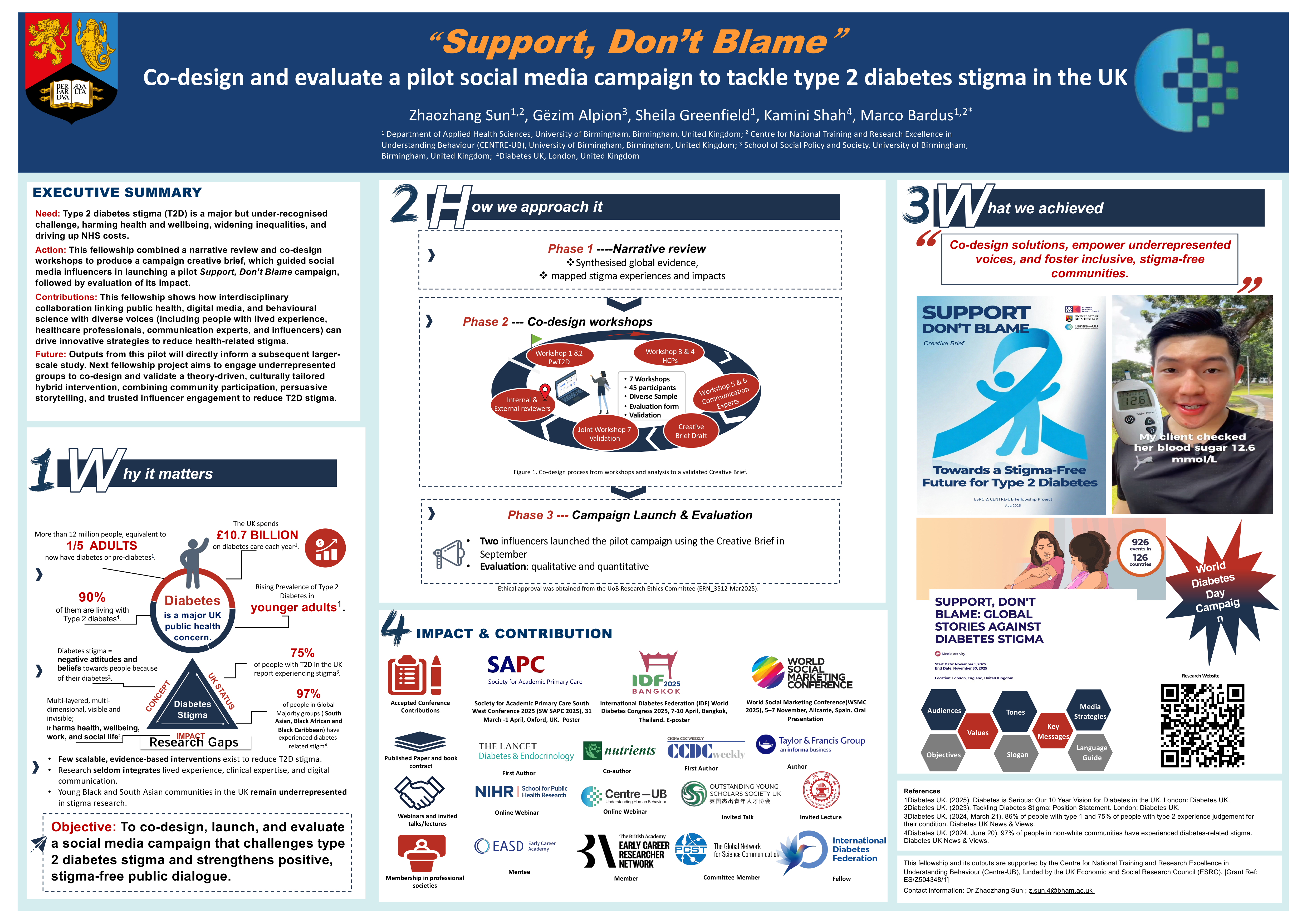
Zhaozhang Sun, University of Birmingham
| Co-authors: | Gezim Alpion, Kamini Shah, Sheila Greenfield, Hannah, Greer, Marco Bardus |
Background
Stigma associated with type 2 diabetes (T2D) harms emotional wellbeing, self-management and engagement with care, particularly among people already disadvantaged by racism, poverty or gendered expectations. Public communication still often presents T2D as the result of poor individual choices. This project presents the co-design, implementation and early evaluation of “Support, Don’t Blame”, a social media campaign developed to promote more compassionate, stigma-reducing narratives about T2D.
Methods
In May 2025, six participatory online workshops were held with 45 stakeholders in the United Kingdom, including people living with T2D, diabetes-related healthcare professionals and communication or marketing experts from health and diabetes organisations. Data from transcripts, chat and Mentimeter were analysed using reflexive thematic analysis to co-produce a campaign handbook. A follow-up online workshop in August 2025 validated and finalised the framework. The handbook was then shared with volunteer social media influencers, who produced campaign content under the agreed title “Support, Don’t Blame”. These materials were evaluated qualitatively through focus groups with people living with T2D and quantitatively through social media analytics.
Results
Co-design identified key principles for anti-stigma content, including acknowledging social and structural drivers of T2D, avoiding moralising language about weight and “control”, highlighting people’s efforts and inviting allies to offer support rather than judgement. Influencer-generated content following the handbook was perceived by focus group participants as more relatable and less blaming than typical health messaging, and achieved promising online engagement in pilot testing.
Conclusion
Partnering with people affected by T2D, health and communication professionals, and influencers can generate content that challenges blame, foregrounds support and remains feasible for campaign delivery. The “Support, Don’t Blame” handbook and campaign provide a transferable model for organisations seeking to address T2D stigma through strategic use of social media.
P Hari Chandran
I am Hari Chandran, a cricket enthusiast who turned my passion into a profession despite battling physical and financial hardships.
At the age of 8, I was struck by polio, which left me immobile and bedridden for nearly two years. With limited resources, my family struggled, but I was determined to fight back. After undergoing surgery on my hands and legs, I gradually regained mobility. Though my dream of pursuing higher education was out of reach due to our financial condition, my love for cricket burned brightly.
Driven by this passion, I sought out cricket associations for differently-abled individuals and became a player. For three consecutive years, I proudly represented the Tamil Nadu state cricket team for the physically challenged. However, my journey was cut short when my body could no longer withstand the physical strain. During one match, I experienced a severe blackout and was rushed to the hospital, where I was diagnosed with Type 1 diabetes, with my blood glucose level soaring to 900 mg/dl.
I was diagnosed with Type 1 diabetes at the age of 23. Managing diabetes was especially difficult due to the weakness in my hands caused by polio. Since my illiterate mother couldn’t administer insulin, my maternal aunt stepped in to help with the injections. Even then, my sugar levels remained high, and my HbA1c reached 16%. In search of better management options, I browsed the Internet and discovered the Tamil Nadu Type 1 Foundation. They introduced me to the Idhayam Charitable Trust in Coimbatore, which provided me with a free insulin pump, significantly improving my condition.
Though my cricketing career as a player came to a halt, my unwavering spirit caught the attention of the association. Recognizing my dedication, they offered me the role of team manager for the Indian cricket team for the physically challenged. This opportunity allowed me to continue contributing to the sport I loved.
To support my family, I work as a vegetable seller in the market, but my cricket commitments limit me to working only three days a week. Managing diabetes with an irregular income was a major challenge, as I often missed insulin doses due to a lack of money, which worsened my health. However, with proper diabetes education and support from Dr. Mohan’s hospital, I learned to manage my condition effectively.
Today, I travel nationally and internationally with the team, winning matches against various countries. The journey has been filled with hurdles, but my love for cricket and relentless determination have helped me achieve my dreams. I am deeply grateful to everyone who supported me in conquering my challenges and enabling me to live my passion.
Salih Hendricks, Dedoc
This narrative explores a 43-year journey of living with diabetes and its complications, highlighting the profound impact of stigma and discrimination on physical health, mental wellbeing, and social identity. My story begins in 1982 with a diagnosis of Diabetes Insipidus, a rare condition that shaped much of my early experiences of misunderstanding and judgment. By age 25, vision-threatening complications led to laser treatments that saved my sight but reinforced the isolating emotional burden of chronic illness. Over the years, I faced kidney complications, artery disease, lens replacements, and a major amputation in 2020, followed by a stroke in 2024. Each complication deepened the stigma projected onto me by society, healthcare systems, and the workplace.
The greatest harm I experienced did not come from diabetes itself, but from the stigma that framed my complications as personal failure. This stigma ultimately led to losing my job, reinforcing how discrimination continues to shape the lives of people living with chronic illness and disability. Through these experiences, I learned that stigma can disable a person more severely than any medical condition.
However, this story is also one of transformation. I broke the silence by sharing my lived experiences publicly, turning decades of hurt, pain, and tears into purpose. Through storytelling, advocacy, and community engagement, I reclaimed my identity and used my journey to challenge societal misconceptions about diabetes. My story illustrates how acknowledging the humanity behind chronic illness can reshape public perception and drive meaningful change.
This abstract offers lived-experience insight into the emotional, cultural, and structural dimensions of diabetes stigma, emphasizing the urgent need for global action to create environments where individuals with chronic conditions are understood, supported, and valued.
Heather Jacobs
Words are powerful, especially when spoken by healthcare providers. Labels like “diabetic,” “uncontrolled,” or “brittle” are not only unhelpful — they can be exceedingly harmful.
At age eight, I awoke from a coma to be told I had “brittle juvenile-onset diabetes” and would not live past forty. Blindness, amputation, and dialysis were presented as inevitable. That message became my expiration date.
I resented being called “brittle.” My identity was rooted in being tough. Yet the dire prognosis left me hopeless. By adolescence, I sought control by setting a goal to be dead by thirty. For more than two decades, I sabotaged my health, convinced my fate was sealed. Appointments only reinforced this cycle: I was scolded for being “non-compliant” and threatened with complications. No one asked why I disregarded care—that I had no hope for anything beyond an abbreviated, miserable life.
Through therapy, I unpacked decades of stigma and learned to forgive the practitioners who lacked awareness of the power of their words. My journey revealed a critical truth: language shapes identity, behavior, and resilience. Fear tactics and judgment-laden terms reduce humans to conditions. Person-centered language fosters empowerment, connection, and hope.
We are humans first. Emotional wellbeing is as vital as physical health. Words can wound, but they can also heal. By choosing language that respects lived experience, healthcare providers can dismantle stigma and inspire action.
Anita Sabidi, DIID
Diabetes Complications Stigma, storytelling in a poem form.
Heather Verry, Diabetes New Zealand
| Co-authors: | Jo Chapman |
Background
Since 2015, Diabetes New Zealand has held Diabetes Action Month annually to raise awareness and educate the public. Each campaign amplifies the voices of people living with diabetes. In 2018, stigma became a key focus through the first Diabetes NZ Stigma Survey, exploring its impact across family, school, work, and social life.
Method
The 2018 campaign, Act Now To Live Well, highlighted the social cost of diabetes. Diabetes NZ partnered with the Australian Centre for Behavioural Research in Diabetes to adapt validated questionnaires and added demographic questions. The survey, distributed online via eDM, captured experiences from 824 respondents with type 1 and type 2 diabetes. Findings informed campaign messaging and future campaigns.
Outcomes
The stigma survey provided valuable insight into the emotional burden of diabetes, resonating with the community and media. Interest was high, as diabetes stigma had been little known until then. Key findings included:
The 2018 campaign generated 218 media items and reached over 300,000 individuals.
In 2020, Love Don’t Judge raised awareness of diabetes distress and its emotional and mental health impacts, reaching millions of New Zealanders through multiple platforms.
In 2024, Don’t Sugar Coat Diabetes, aimed to dispel myths, reduce stigma, and encourage Kiwis to understand and check their risk of type 2 diabetes.
Community involvement remains central, with people with lived experience sharing stories, appearing in videos, and engaging with media.
Kamlesh Chitte, UDAAN for Children with Diabetes, Maharashtra
Background / Aim
For a rural girl in India, a Type 1 Diabetes (T1D) diagnosis is not only a medical condition — it becomes a lifelong social restriction. She is labelled “weak,” confined at home, removed from sports, protected from friendships, and quietly judged as “unfit” for marriage, work, or motherhood. Stigma shapes every decision others make about her body and her future.
This initiative aimed to confront this deeply gendered stigma and document the long-term impact of community-based support on rural girls’ education, mobility, identity, and life outcomes.
Methods
Across 25 years, over 1500+ rural girls with T1D participated in layered stigma-reduction activities within UDAAN’s peer-support environment, a safe space that allowed girls to be seen, heard, and believed.
Interventions targeted the exact points where stigma is enforced:
Role models, peer circles, and community sensitisation formed the emotional backbone of the program.
Outcomes
The initiative produced measurable shifts:
Lessons Learned
Gender-based stigma cannot be dismantled by information alone. It requires emotional safety, community solidarity, and lived-experience leadership. When rural girls receive long-term support as they did within UDAAN they rise beyond stigma and reshape cultural norms themselves.
Meaningful Involvement of Lived Experience
Girls and young women living with T1D co-created peer activities, designed the messaging, led community sessions, and shaped the entire approach. Their experiences were not included they led the change.
Anmol Budhiraja, Diabetes Action Canada (DAC)
| Co-authors: | Jeremy Auger |
Background / Aims(s)
This project is part of the Diabetes Action Canada Research-to-Action Fellowship in partnership with the Indigenous Diabetes Health Circle (IDHC). Community members described being misdiagnosed, having tests delayed and feeling dismissed in appointments—experiences that disproportionately affect Indigenous, Black and Brown people. Our aim is to create practical, culturally grounded tools that help people recognise symptoms, ask for essential tests and assert their rights in clinical settings.
Methods (Who, What, Where)
Together with IDHC, we held a co-design session with over two dozen Indigenous, Black and Brown participants who had lived or loved experience of diabetes or had supported family through misdiagnosis. Sharing Circles explored how racism, weight stigma and stereotypes about “who gets diabetes” shaped care and silenced questions.
Using participants’ words, we drafted “Diabetes Answers for Us” wallet cards listing common symptoms, key tests and plain-language rights for medical appointments. A short follow-up survey invites wider feedback and offers people the chance to review drafts before finalisation
Outcomes (achieved or expected)
The wallet cards and a companion easy-to-read guide will be freely available through Diabetes Action Canada and IDHC in early 2026. We expect them to provide discreet, portable support that increases confidence to ask for tests, helps people connect symptoms to diabetes and enables them to challenge biased or dismissive care in real time.
Lessons Learned (for scaling / adaptation)
Co-design confirmed that shame around diabetes and misdiagnosis is cultural and systemic, not personal. Low-barrier tools like wallet cards can interrupt that shame by giving people accessible language and questions. Grounding the tools in Indigenous, Black and Brown voices, plain language and low-tech design offers a model for adapting this work to other racialized and diaspora communities, including future versions for India.
Description of how people with lived experience are / have been meaningfully involved
The project is led by two Fellows whose lived, loved, learned and laboured experience spans type 1 diabetes, a new type 2 diagnosis, Indigenous identity, Indian diaspora identity, family caregiving and chronic-disease work. The co-design session with more than two dozen community members shaped every stage—from identifying systemic barriers and emotional triggers to deciding which rights, symptoms and tests to include. Their insights continue to guide the wording, visuals and evaluation of the final tools, ensuring they reflect real needs and restore agency in care.

Chris Bright, The Diabetes Football Community
Background / Aims(s)
Diabetes stigma negatively affects mental health, confidence, and participation in physical activity. The Diabetes Football Community (TDFC) was created to challenge these barriers by using football and futsal as vehicles for inclusion, education, and empowerment. Its aim is to normalise diabetes management in sport, reduce stigma, and foster peer support networks.
Methods (Who, What, Where)
Established in 2017, TDFC delivers grassroots football events, futsal tournaments, and educational projects across the UK and internationally. Activities include in-person training sessions, competitive fixtures, and digital engagement through social media, podcasts, and webinars. The community is open to people living with diabetes, their families, and supporters, creating safe spaces for shared learning and participation.
Outcomes (Achieved or Expected)
TDFC has reached thousands globally, with over 10,000 social media followers and hundreds attending events annually. Participants report improved confidence in managing diabetes during exercise, reduced feelings of isolation, and enhanced mental wellbeing. Educational content has supported healthcare professionals and coaches, increasing understanding of diabetes in sport and reducing misconceptions. TDFC’s advocacy has influenced policy discussions and inspired similar initiatives nationally and internationally.
Lessons Learned (Scaling or Adaptation)
Sport is a powerful tool for stigma reduction, but scaling requires strong partnerships with healthcare providers, sports governing bodies, and diabetes charities. Digital platforms have proven essential for global reach and sustainability, while co-design with community members ensures relevance and authenticity. Future adaptation will focus on expanding resource accessibility and integrating TDFC’s model into mainstream football structures.

Mohammed Ashraf, Diabetes Action Canada
| Co-authors: | Amanda Knight |
Background / Aims(s)
Diabetes technologies, such as insulin pumps and automated insulin delivery (AID) systems, ease care burdens, yet many users feel intimidated or judged as “not good enough” for these technologies. Here, we aim to reduce stigma around diabetes technology by creating an artificial intelligence (AI)-powered pump and AID chatbot navigator that offers an individualized space to ask sensitive questions, fostering confident shared decision-making with healthcare teams.
Methods
Through the Diabetes Action Canada Research-to-Action Fellowship program, two fellows with lived and loved experience of type 1 diabetes (T1D) led a co-design session with over two dozen people with diabetes and caregivers. Participants shared “heaviest” unasked questions from clinic or tech support groups, highlighting stigma from external and diabetes community sources that make technology feel inaccessible or unsafe. Session insights shaped the chatbot for four persona types (lived, loved, learned, and labored experience); using verified AID manufacturer guides and summaries; separating Canadian and United States (US)-specific information; offering grade 3‒5 reading level explanations; and avoiding recommendations, pricing, or medical advice.
Outcomes (achieved or expected)
Early user data informs rehearsing difficult questions about eligibility, safety, everyday use, and funding before clinic visits. A private space to explore “embarrassing” questions helps reduce shame and prepare technological options discussions with care teams. Expected outcomes include increased confidence in addressing diabetes technology-related questions, equitable access to geography-specific information, and identification of stigma-related themes to guide future education and advocacy efforts.
Lessons Learned (for scaling/adaptation)
Stigma extends beyond clinics into peer and tech support spaces. Participants described feeling judged for using or not using a particular system. Scaling requires ensuring anonymous, judgment-free tools for testing questions; relying on transparent, trusted information sources; separating country-specific content; and using simple, non-hierarchical devices or user comparisons. These elements adapt the tool to other regions and technologies while prioritizing stigma reduction.

Temboh Alomba, Reconciliation And Development Association – RADA
| Co-authors: | Moffo Anaisse; Mbiydzenyuy Sonyuy |
Background / Aims(s)
The T1D Picnic addressed the psychosocial challenges faced by children and adolescents living with Type 1 Diabetes (T1D) in the Northwest Region of Cameroon, where late diagnosis, stigma, emotional distress, and caregiver burnout hinder effective disease management. The aim was to enhance emotional wellbeing, coping capacity, and social connectedness through a structured two-day psychosocial support picnic.
Methods
Implemented by RADA, the intervention brought together children with T1D and their caregivers in a therapeutic community setting. Activities included Cognitive Behavioral Therapy (CBT), sight-seeing, emotional support circles, peer discussions, art therapy, and experiential learning sessions. Pre- and post-test assessments using 5‑point Likert scales measured stress, anxiety, stigma, emotional regulation, coping, communication, burnout, and social wellbeing.
Outcomes
Children showed improved confidence and reduced disclosure challenges, with gradual strengthening of coping skills and quality of life. Caregivers demonstrated better communication, emotional support, and social wellbeing. Emotional shifts such as increased awareness of stigma among children and temporary emotional fatigue among caregivers were expected as part of early psychosocial adjustment.
Lessons Learned
Psychosocial support is essential for comprehensive diabetes management. Creating safe spaces for emotional expression reduces isolation and strengthens resilience. Early emotional turbulence is normal, highlighting the importance of continuous follow‑up. The model is scalable across similar low‑resource settings.
Involvement of People with Lived Experience
Children with T1D and their caregivers actively shaped discussions, identified priority challenges, co‑created coping strategies, and shared lived experiences. Their insights informed the design, delivery, and evaluation of the intervention, ensuring relevance and community ownership.
Sana Ajmal, Meethi Zindagi
| Co-authors: | Muhammadah Khalid; Anum Anwar |
Background
Children and adolescents with Type 1 Diabetes (T1D) in Pakistan face a double burden: the daily challenges of managing their condition and the pervasive social stigma of being labeled “untouchable” or “abnormal.” Such experiences silently corrode self-belief, extinguish their spark, and push children into deep social isolation. Despite this burden, Pakistan has had no structured, community-based intervention directly addressing T1D-related stigma.
Objective
This study documents Pakistan’s first structured stigma-reduction initiative the Buddy System, led by Meethi Zindagi (MZ), combining peer support, culturally tailored diabetes education, and person-centered counselling. We aimed to understand the lived experiences of stigma among children with T1D and assess the early impact of MZ’s support approach.
Methods
Several in-depth case studies were conducted with children aged 8–17 who experienced school discrimination, friendship abandonment, family blame, and social withdrawal due to T1D. Narrative interviews with children and caregivers were complemented with field observations by MZ educators and researchers. Trained T1D peer leaders conducted home and community visits, intentionally bringing a small “gift of interest” (e.g., drawing book, football, storybook) to build trust, reduce fear of communication, and bridge the emotional gap between buddies and mentors. Thematic analysis examined stigma triggers, emotional consequences, and pathways of support.
Results
Narratives revealed recurrent themes of social shaming, fear of injecting insulin publicly, peer exclusion, and internalized stigma. MZ’s intervention offered safe emotional space, consistent mentoring, caregiver engagement, and accessible, culturally relevant education. Children reported increased confidence in self-management, re-engagement in school, and reduced fear of disclosure. Families noted improved acceptance and stronger coping capacity.
Conclusion
T1D-related stigma in Pakistan is a neglected barrier that deepens emotional distress and disrupts diabetes care. Engagement with trained mentors helped children remain connected, and many expressed the desire for follow-up visits every two months to stay motivated. All children in the program have since regained confidence and are now living more empowered, healthier lives. This model underscores the urgent need to integrate psychosocial and anti-stigma support into routine diabetes care.